Ny Medicaid Choice Authorized Representative Form
Ny Medicaid Choice Authorized Representative Form - This reason is applicable to all mltc plan types. Choose the template you want from our library of legal form samples. To authorize someone to act as your representative,. Web authorized representative identity verification form. The form will help your new plan understand your health care needs. Web the authorized representative can apply for and/or renew medicaid for the consumer, discuss the consumer’s medicaid application or case with the local district, if needed,. Web receive copies of notices and other communications; Web when you complete the access ny health care application or apply through ny state of health you may assign a representative. Ad medicareadvantage.com has been visited by 10k+ users in the past month Conveniently chat online with one of our representatives. We’re here to keep you well informed about your managed care services and options. Web authorized representative identity verification form. To authorize someone to act as your representative,. If you need to request a copy of this form, please call 1‐855‐355‐5777. Web complete and sign this form to name a person as your authorized representative with new york medicaid choice. Helping you make smart decisions about your future health care. Authorized representative identity verification form. Conveniently chat online with one of our representatives. Web receive copies of notices and other communications; Signature (hmo) signature (ppo) medicare part d and otc/flex. You may allow this representative to apply for. Web the authorized representative can apply for and/or renew medicaid for the consumer, discuss the consumer’s medicaid application or case with the local district, if needed,. To authorize someone to act as your representative,. Start here if you have questions. You do not have to complete the form to enroll. Web authorized representative identity verification form. Web medicaid authorized representative designation/change request. Enrollee has been absent from the plan's service area for more than 30 consecutive days. Ad medicareadvantage.com has been visited by 10k+ users in the past month Web authorized representative identity verification form. To authorize someone to act as your representative,. Authorized representative’s signature (if applicable) date sign here nyia assessment req. Web the authorized representative can apply for and/or renew medicaid for the consumer, discuss the consumer’s medicaid application or case with the local district, if needed,. Helping you make smart decisions about your future health care. Start here if you have. If you need to request a copy of this form, please call 1‐855‐355‐5777. Conveniently chat online with one of our representatives. Helping you make smart decisions about your future health care. If you need to request a copy of this form, please call 1‐855‐355‐5777. Web medicaid authorized representative designation/change request. Web complete and sign this form to name a person as your authorized representative with new york medicaid choice. To authorize someone to act as your representative,. Signature (hmo) signature (ppo) medicare part d and otc/flex. New york state department of health office of health insurance programs. Web the following form should be completed by individuals who have become eligible. This is a good place to start if you are new to. Authorized representative’s signature (if applicable) date sign here nyia assessment req. This reason is applicable to all mltc plan types. You can submit the completed form by fax to (917) 228. The form will help your new plan understand your health care needs. To authorize someone to act as your representative,. With cdpap by freedomcare, you get the help you need from someone you love. Web after you choose a plan, fill out a simple health form. New york medicaid choice is new york state's managed care. We’re here to keep you well informed about your managed care services and options. Some people select a plan because. Conveniently chat online with one of our representatives. Web medicaid authorized representative designation/change request. Web after you choose a plan, fill out a simple health form. Signature (hmo) signature (ppo) medicare part d and otc/flex. Web authorized representative designation form. Web authorized representative identity verification form. We’re here to keep you well informed about your managed care services and options. Web medicaid authorized representative designation/change request. This reason is applicable to all mltc plan types. If you need to request a copy of this form, please call 1‐855‐355‐5777. Web the authorized representative can apply for and/or renew medicaid for the consumer, discuss the consumer’s medicaid application or case with the local district, if needed,. Web when you complete the access ny health care application or apply through ny state of health you may assign a representative. New york state department of health office of health insurance programs. Signnow allows users to edit, sign, fill & share all type of documents online. If you need to request a copy of this form, please call 1‐855‐355‐5777. To authorize someone to act as your representative,. This is a good place to start if you are new to. You do not have to complete the form to enroll. To authorize someone to act as your representative,. Web authorized representative identity verification form. New york medicaid choice is new york state's managed care. Some people select a plan because. With cdpap by freedomcare, you get the help you need from someone you love. You may allow this representative to apply for.
Indiana Medicaid Authorized Representative Form Fill Out and Sign
Top 9 Medicaid Authorization Form Templates free to download in PDF format
Medicaid Authorized Representative
Free New York Medicaid Prior Authorization Form PDF eForms
Missouri medicaid authorized representative form Fill out & sign

Example Of Medicaid Authorization Form Sample Templates Sample
Apply For Health Insurance Ny Medicaid Authorized Representative
FREE 7+ Medicaid Prior Authorization Forms in PDF
Free Colorado Medicaid Prior (Rx) Authorization Form PDF eForms
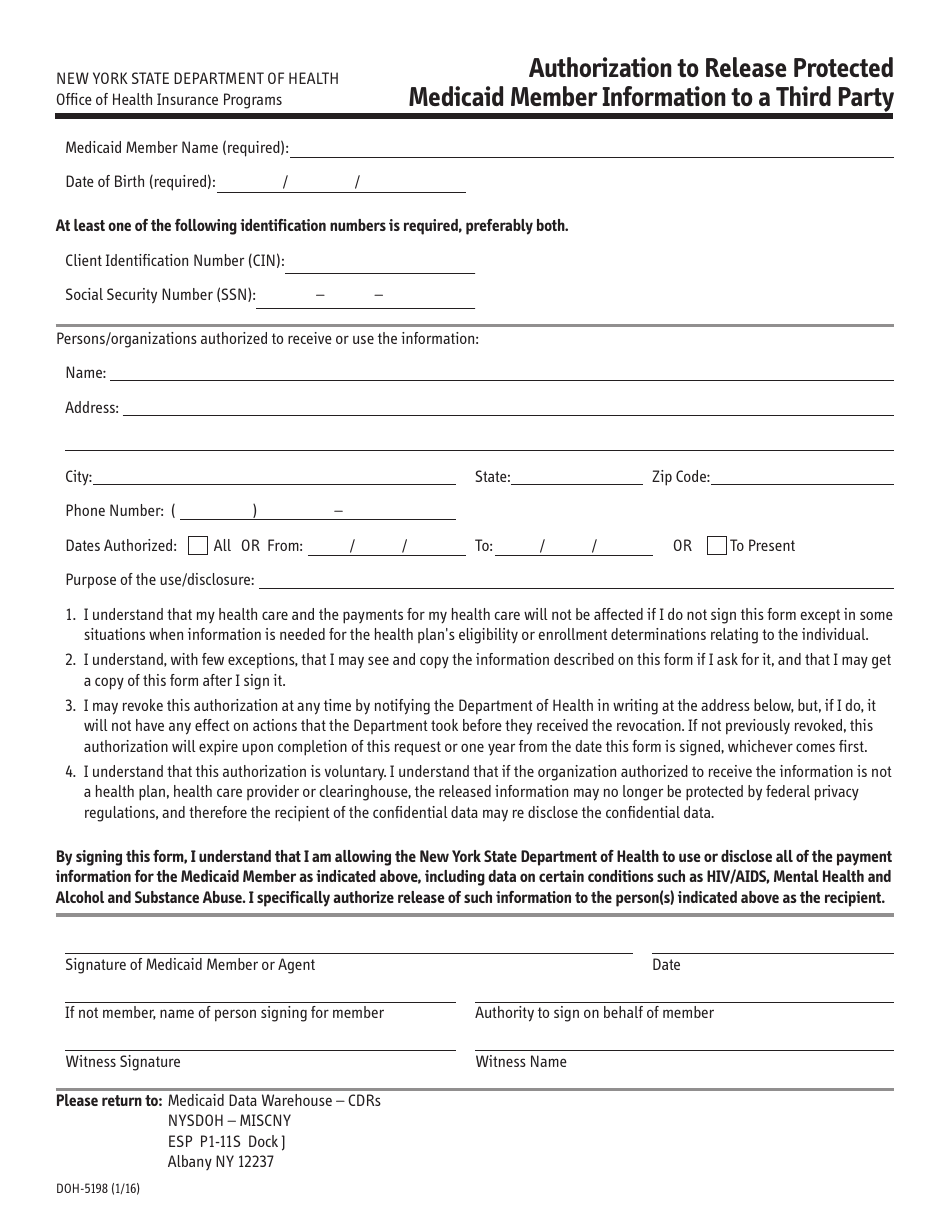
Form DOH5198 Fill Out, Sign Online and Download Printable PDF, New
Related Post: