Ambetter Appeal Form
Ambetter Appeal Form - General new century health information. Web confidentiality access to your records documentation for an appeal filing complaint with the adoi receipt of documents member appeals packet access all member appeals. Web you file an appeal in response to a denial received from ambetter from health net. You must file an appeal within 180 days of the date on the denial letter. There, you can find information about your ambetter coverage,. Use your zip code to find your personal plan. Web provider complaint/grievance and appeal process. Web you may file an appeal by phone, fax, or in person. 1) a copy of the eop(s) with the claim numbers to be adjudicated clearly circled 2) the response to your original request for. If you have questions about your health insurance coverage, we'd love to hear from you. Web the procedures for filing a complaint/grievance or appeal are outlined in the ambetter member’s evidence of coverage. Web grievance or appeal form. Web an appeal is the mechanism which allows providers the right to appeal actions of ambetter such as a prior authorization denial, or if the provider is aggrieved by any rule, policy or. For urgently needed services. Web grievance or appeal form. 1) a copy of the eop(s) with the claim numbers to be adjudicated clearly circled 2) the response to your original request for. Web an appeal is the mechanism which allows providers the right to appeal actions of ambetter such as a prior authorization denial, or if the provider is aggrieved by any rule, policy. Web the azch appeals process consists of the following levels of review: Web you may file an appeal by phone, fax, or in person. Web provider reconsideration and appeal request form (pdf) covermymeds guide (pdf) update and certify provider data in cms's nppes (pdf) ambetter from home state. Web a claim dispute/claim appeal must be submitted on this claim dispute/appeal. Web provider complaint/grievance and appeal process. Web provider reconsideration and appeal request form (pdf) covermymeds guide (pdf) update and certify provider data in cms's nppes (pdf) ambetter from home state. Web grievance or appeal form. Web confidentiality access to your records documentation for an appeal filing complaint with the adoi receipt of documents member appeals packet access all member appeals.. General new century health information. Claim complaints must follow the dispute process and then the complaint process below. All fields are required information. Web to ensure that ambetter member's rights are protected, all ambetter members are entitled to a complaint/grievance and appeals process. Web provider complaint/grievance and appeal process. If you have questions about your health insurance coverage, we'd love to hear from you. Use this form to request one of the following: Web what is ambetter health? Web to ensure that ambetter member's rights are protected, all ambetter members are entitled to a complaint/grievance and appeals process. This could be a denial of coverage for requested medical care. The procedures for filing a. For urgently needed services not yet provided: Ambetter network providers deliver quality. Web the procedures for filing a complaint/grievance or appeal are outlined in the ambetter member’s evidence of coverage. All fields are required information. See coverage in your area; General new century health information. For urgently needed services not yet provided: Use your zip code to find your personal plan. Web confidentiality access to your records documentation for an appeal filing complaint with the adoi receipt of documents member appeals packet access all member appeals. Web an appeal is the mechanism which allows providers the right to appeal actions of ambetter such as a prior authorization denial, or if the provider is aggrieved by any rule, policy or. If you wish to file a grievance or an appeal, please complete this form. All fields are required information. Web your ambetter online member account is a. For urgently needed services not yet provided: Web confidentiality access to your records documentation for an appeal filing complaint with the adoi receipt of documents member appeals packet access all member appeals. Web what is ambetter health? Web the azch appeals process consists of the following levels of review: Web provider reconsideration and appeal request form. Web provider reconsideration and appeal request form (pdf) covermymeds guide (pdf) update and certify provider data in cms's nppes (pdf) ambetter from home state. For urgently needed services not yet provided: All fields are required information. Web provider complaint/grievance and appeal process. If you wish to file a grievance or an appeal, please complete this form. You must file an appeal within 180 days of the date on the denial letter. Web you may file an appeal by phone, fax, or in person. Use this form to request one of the following: The procedures for filing a. Web you file an appeal in response to a denial received from ambetter from health net. Use your zip code to find your personal plan. Web grievance or appeal form. If you choose not to complete this form, you may write a letter that includes. 1) a copy of the eop(s) with the claim numbers to be adjudicated clearly circled 2) the response to your original request for. The claim dispute form must be completed in its. There, you can find information about your ambetter coverage,. Claim complaints must follow the dispute process and then the complaint process below. If you have questions about your health insurance coverage, we'd love to hear from you. The completed form can be returned by mail or fax. Web the azch appeals process consists of the following levels of review:
What Is The Group Id For Ambetter Member ID Cards Healthy Kids

US Court of Appeals Criminal Appeal Information Sheet Complete Legal

20202022 CA OSHAB Appeal Form 100 Fill Online, Printable, Fillable
Ambetter Prior Auth Form 2020 Fill and Sign Printable Template Online
Nics Voluntary Appeal Form eversilicon
Amerigroup change pcp Fill out & sign online DocHub
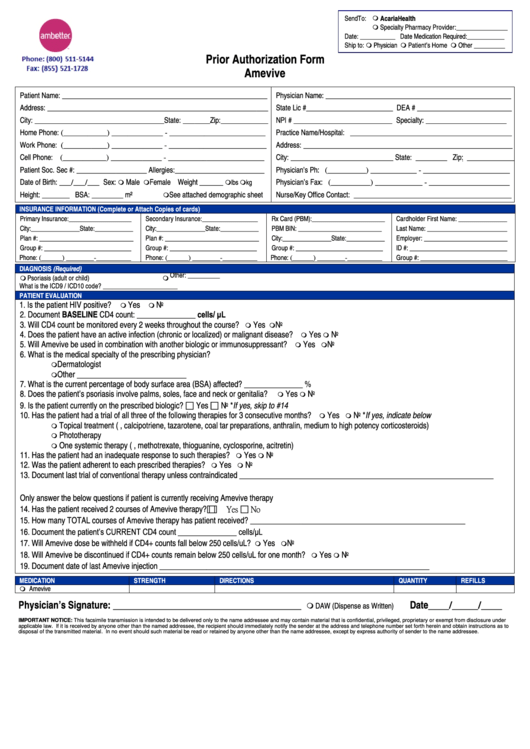
Ambetter Prior Authorization Form Amevive printable pdf download
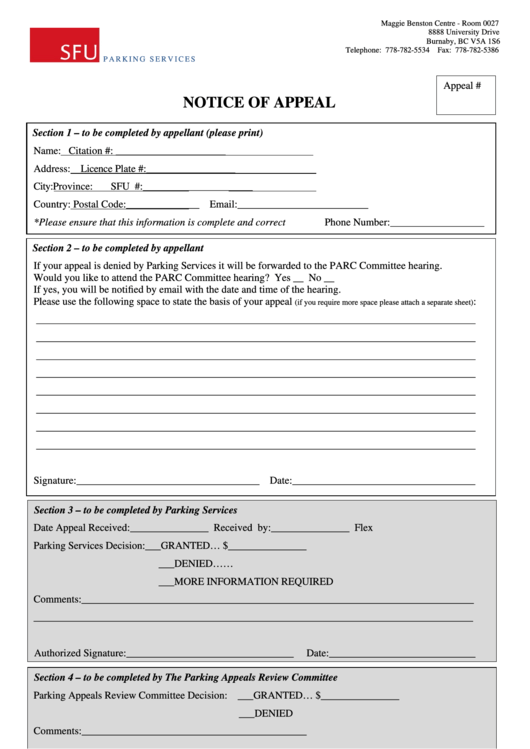
Fillable Notice Of Appeal Form printable pdf download
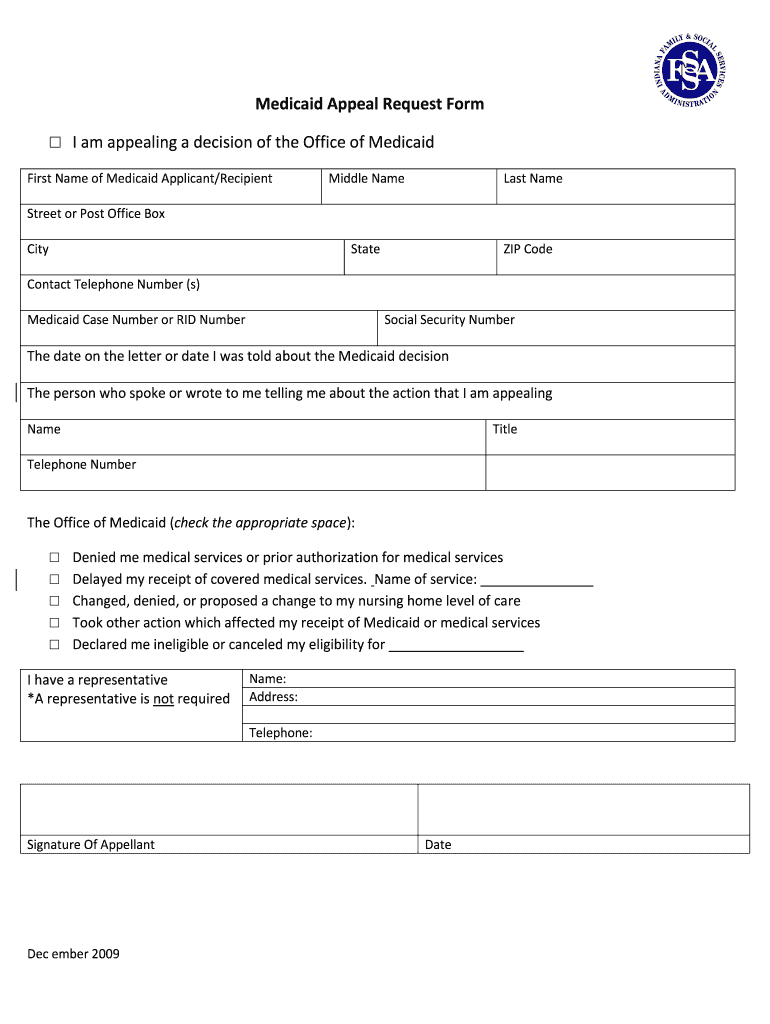
Indiana Medicaid Appeal Form Fill Online, Printable, Fillable, Blank
Ambetter Superior Health Plan Appeal Form
Related Post: