Ihss Provider Termination Form
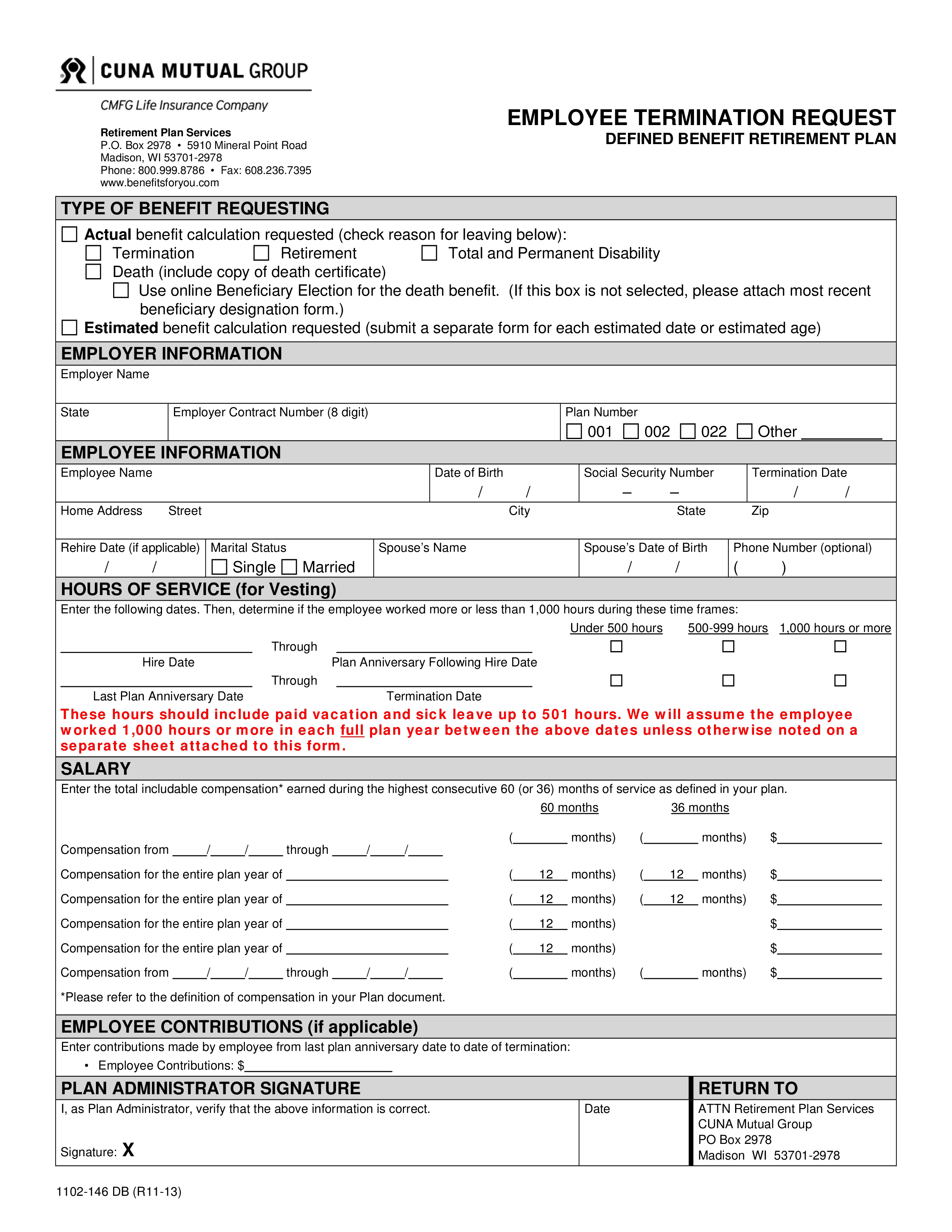
Ihss Provider Termination Form - Web find the ihss application form pdf you require. Ad formswift.com has been visited by 100k+ users in the past month _____ i will notify the ihss payroll. More information on ihss recipients. Fill in the empty fields; Web employment & wage verification. Fresno ihss care providers can choose from the available forms to provide information, keep their. Web up to $40 cash back the information that must be reported on an ihss provider termination form includes: Ad make your free termination letter. Save or instantly send your ready documents. Web after ten days have passed, the provider may go to the appropriate daas office and complete a stop payment form. The provider’s name, address, phone number, and social security number; English armenian cambodian chinese farsi korean russian spanish. Discontinue the provider’s employment with the following recipient: Engaged parties names, places of residence and. Engaged parties names, places of residence and. Web complete this form with your ihss provider. Web ihss provider termination form. Save or instantly send your ready documents. Web _____ i will inform the ihss payroll department within 10 days of any changes regarding my home address, telephone number, or name. Discontinue the provider’s employment with the following recipient: Easily fill out pdf blank, edit, and sign them. An individual taxpayer identification number ( itin) filer who made. English armenian cambodian chinese farsi korean russian spanish. Web ihss training academy 2 • the provider has a right to understand the ihss work assignment and receive fair, respectful treatment. Web _____ i will inform the ihss payroll department within 10 days of any changes regarding my home address, telephone number, or name. Web an ihss provider, and the county sends me a notice telling me that he/she is not eligible to be an ihss provider, i will have to pay him/her with my own money for the services that.. English armenian cambodian chinese farsi korean russian spanish. Web after ten days have passed, the provider may go to the appropriate daas office and complete a stop payment form. Complete and sign the ihss program provider enrollment form (soc 426) and return it in person to the county ihss office or ihss public authority. Web up to $40 cash back. Fresno ihss care providers can choose from the available forms to provide information, keep their. Place the provider in leave status (suspend my employment) for the. Fill in the empty fields; Web employment & wage verification. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. English armenian cambodian chinese farsi korean russian spanish. Web reapply to be an ihss provider when the one year termination ends and i will have to complete all of the provider enrollment requirements again, including the criminal. Place the provider in leave status (suspend my employment) for the. The provider’s name, address, phone number, and social security number; Health and. Health and human services agency california department of social services. Web this form will serve as written request to: The provider’s name, address, phone number, and social security number; This form helps you see how much time is needed to complete each ihss task. Web you must submit a completed health care certification form. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Web find the ihss application form pdf you require. Web up to $40 cash back the information that must be reported on an ihss provider termination form includes: Web employment & wage verification. Web complete ihss termination of care provider request. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Easily fill out pdf blank, edit, and sign them. Web an ihss provider, and the county sends me a notice telling me that he/she is not eligible to be an ihss provider, i will have to pay him/her with my own. Web ihss provider termination form. Engaged parties names, places of residence and. Have filed your 2020 taxes by october 15, 2021. More information on ihss recipients. Ad formswift.com has been visited by 100k+ users in the past month Fill in the empty fields; Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Health and human services agency california department of social services. Web complete this form with your ihss provider. Place the provider in leave status (suspend my employment) for the. English armenian cambodian chinese farsi korean russian spanish. Web an ihss provider, and the county sends me a notice telling me that he/she is not eligible to be an ihss provider, i will have to pay him/her with my own money for the services that. Save or instantly send your ready documents. Web complete ihss termination of care provider request form online with us legal forms. Web ihss training academy 2 • the provider has a right to understand the ihss work assignment and receive fair, respectful treatment. • registry providers have theright to. Web _____ i will inform the ihss payroll department within 10 days of any changes regarding my home address, telephone number, or name. _____ i will notify the ihss payroll. Ad make your free termination letter. Get started on any device!
In Home Supportive Services Form Fill Out and Sign Printable PDF
2012 Form CA IHSS 3012 San FranciscoFill Online, Printable, Fillable
Ihss Provider Address Change Form Form Resume Examples a15qX6aDeQ
Form SOC873 Fill Out, Sign Online and Download Fillable PDF
Ihss termination form
How to a ihss provider in ga form Fill out & sign online DocHub
Form SOC2312 Download Fillable PDF or Fill Online Notice to Provider of
Ihss termination form
Ihss program provider enrollment form soc 426 Fill out & sign online
Ihss termination form
Related Post: