Federal Blue Cross Blue Shield Claim Form
Federal Blue Cross Blue Shield Claim Form - Edit, sign and save 14150camenab form. Web all forms must be signed, then either faxed or mailed. If this is a compound claim, enter the national drug. Blue cross and blue shield of arizona. Web health benefits claim form. Only claims for prescriptions purchased from a retail pharmacy are to be sent to the address on the front. Claims administrator, po box 14053 lexington, ky 40512. You’ll also be notified immediately when we receive your. Instructions for completing patient and. When you visit a doctor, we pay after we get a claim. Your local company can help you to: Please follow this federal employees health benefits program disputed claims process if you disagree. Web online claims are processed faster and you can conveniently submit them from your computer or mobile device. Web all forms must be signed, then either faxed or mailed. Each claim form must be signed. Web online claims are processed faster and you can conveniently submit them from your computer or mobile device. Instructions for completing patient and. Web health benefits claim form. Please follow this federal employees health benefits program disputed claims process if you disagree. Claims administrator, po box 14053 lexington, ky 40512. For services provided in alaska or washington:. Please complete a separate claim form for each patient and each pharmacy. Claims administrator, po box 14053 lexington, ky 40512. Each claim form must be signed. Web pay me back claim form. Please complete a separate claim form for each patient and each pharmacy. Web pay me back claim form. When you visit a doctor, we pay after we get a claim. Web online claims are processed faster and you can conveniently submit them from your computer or mobile device. Download a claim form for medical services, pharmacy services or overseas care. Download and complete the correct claim form. Web blue cross® and blue shield® service benefit plan fep® blue focus. Please follow this federal employees health benefits program disputed claims process if you disagree. Ad download or email 14150camenab & more fillable forms, register and subscribe now. Web online claims are processed faster and you can conveniently submit them from your. Instructions for completing patient and. We use cookies on this website to give you the best experience and measure website usage, by continuing to use this website, you consent to these cookies. Web all forms must be signed, then either faxed or mailed. Web online claims are processed faster and you can conveniently submit them from your computer or mobile. Web health benefits claim form. Web the disputed claims process. Download and complete the correct claim form. Web when the claim form has been completed and signed, please mail it to your local blue cross and blue shield company. Only claims for prescriptions purchased from a retail pharmacy are to be sent to the address on the front. You’ll also be notified immediately when we receive your. Download and complete the correct claim form. Edit, sign and save 14150camenab form. Blue cross and blue shield of arizona. Web when the claim form has been completed and signed, please mail it to your local blue cross and blue shield company. Web the disputed claims process. Ad download or email 14150camenab & more fillable forms, register and subscribe now. You can use our interactive search to find your local blue cross blue shield company's website. Please follow this federal employees health benefits program disputed claims process if you disagree. Web when the claim form has been completed and signed, please mail. Your local company can help you to: Instructions for completing patient and. You can use our interactive search to find your local blue cross blue shield company's website. Claims administrator, po box 14053 lexington, ky 40512. Web blue cross® and blue shield® service benefit plan fep® blue focus. Ad download or email 14150camenab & more fillable forms, register and subscribe now. Only claims for prescriptions purchased from a retail pharmacy are to be sent to the address on the front. You can use our interactive search to find your local blue cross blue shield company's website. Web the disputed claims process. Claims administrator, po box 14053 lexington, ky 40512. Instructions for completing patient and. Please follow this federal employees health benefits program disputed claims process if you disagree. For services provided in alaska or washington:. Web all forms must be signed, then either faxed or mailed. Edit, sign and save 14150camenab form. Web online claims are processed faster and you can conveniently submit them from your computer or mobile device. Instructions for completing patient and. Web when the claim form has been completed and signed, please mail it to your local blue cross and blue shield company. Each claim form must be signed. When you have completed this form, please include your. Please complete a separate claim form for. Please complete a separate claim form for each patient and each pharmacy. Your local company can help you to: Each claim form must be signed. Claims administrator, po box 14053 lexington, ky 40512.
Blue cross blue shield overseas claim form Fill out & sign online DocHub
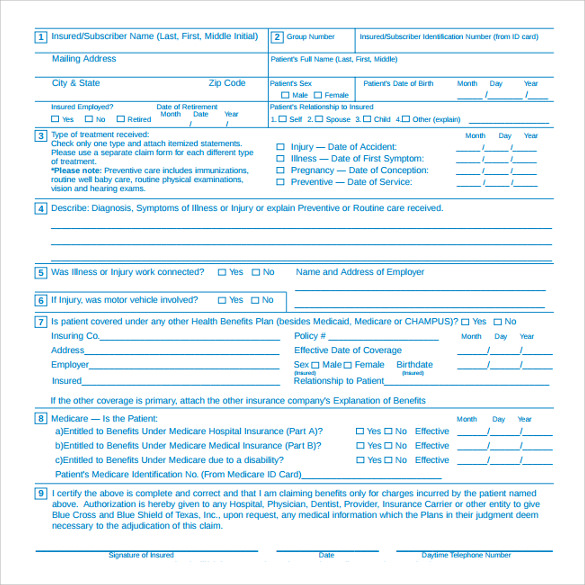
FREE 6+ Sample Medical Claim Forms in PDF
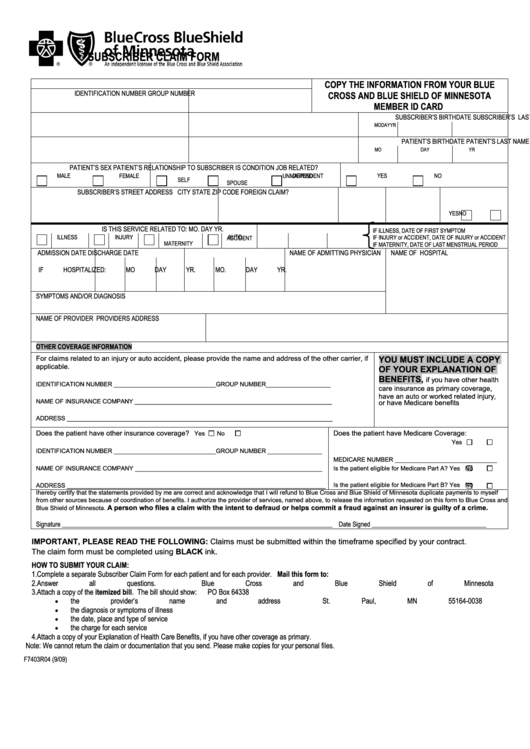
Form F7403r04 Bcbs Subscriber Claim Form printable pdf download
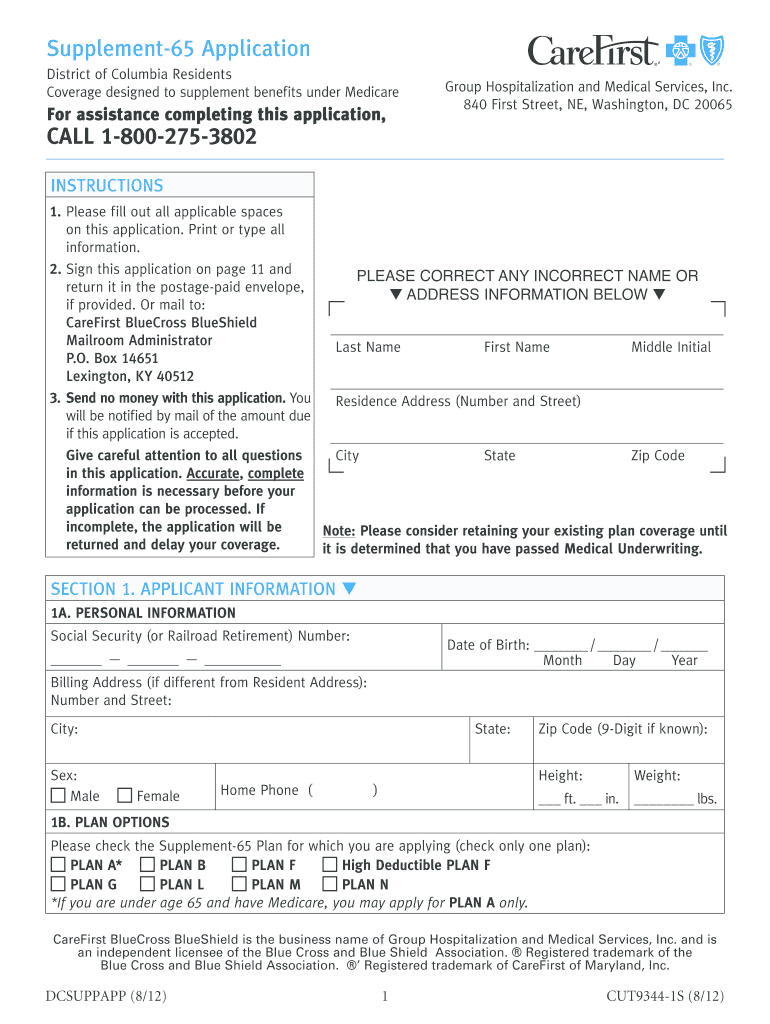
Blue Cross Blue Shield Application Form Fill Out and Sign Printable

federal bcbs basic overseas claim form 2012 Fill out & sign online
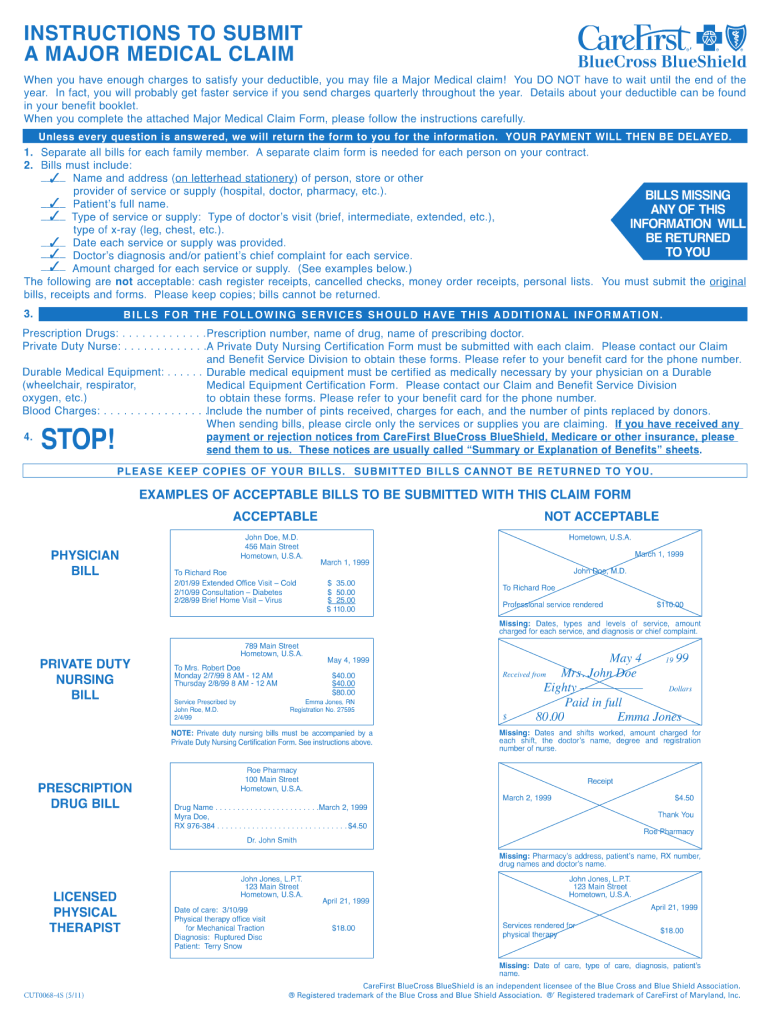
Care First Blue Cross Blue Shield Major Medical Claim Form Fill Out
Document 10391911

Blue Cross Blue Shield Association Member Claim Form PDFSimpli
Anthem claim forms california Fill out & sign online DocHub

Blue cross blue shield anthem eft enrollment form Fill out
Related Post: