Arkansas Medicaid Prior Authorization Form
Arkansas Medicaid Prior Authorization Form - 04/07/2023 arkansas medicaid © 2023 by magellan rx management, llc. When prompted, select 0 for other inquiries, then option 3 for provider enrollment. Most forms are available in section v of your provider manual. Navigate personal care prior authorization form; Web where can i get medicaid forms i need? Arkansas foundation for medical care (afmc) division of medical services attn: The forms below cannot be printed from this manual for use. Others are added as they become available. Web ebrx prior authorization call center phone: Acthar gel (corticotropin injection) prior authorization (pa) request form. Acthar gel (corticotropin injection) prior authorization (pa) request form. Navigate addt/eidt prior authorization form; Web interpreter services request. 0632 — pharmacy multiple sources. Web where can i get medicaid forms i need? The patient must have a diagnosis of relapsing. The following always require prior authorization: When prompted, select 0 for other inquiries, then option 3 for provider enrollment. Confidential and proprietary property of ebrx page 2 of 395 abiraterone (zytiga®) 250 mg tablets. Arkansas medicaid state supplemental rebate contract template. Web through this secure and easy to use internet portal, healthcare providers can submit claims and inquire on the status of their claims, inquire on a patient’s eligibility, upload files containing 837 transactions, and search for another provider. Web where can i get medicaid forms i need? When prompted, select 0 for other inquiries, then option 3 for provider enrollment.. Navigate addt/eidt prior authorization form; Relapsing forms of multiple sclerosis (rrms) criteria 1. The patient must have a diagnosis of relapsing. 04/07/2023 arkansas medicaid © 2023 by magellan rx management, llc. Acthar gel (corticotropin injection) prior authorization (pa) request form.pdf jun 28, 2023 8:06:12 pm Hospital or ambulatory surgery center name. Web ebrx prior authorization call center phone: Please attach or include a letter of medical necessity along with supporting documentation (e.g. This model of care was developed to address the overall health care needs of medicaid beneficiaries who have complex behavioral health or intellectual and developmental disability (idd) service needs. The forms below cannot. When prompted, select 0 for other inquiries, then option 3 for provider enrollment. Others are added as they become available. A repository of medicare forms and documents for wellcare providers, covering topics such as authorizations, claims and behavioral health. Navigate personal care prior authorization form; Arkansas medicaid state supplemental rebate contract template. The patient must have a diagnosis of relapsing. In addition, healthcare providers can use this site to locate claim forms, provider participation. Navigate community based outpatient prior authorization form; Learn more the official website of the state of arkansas The provider may request a supply of this claim form from any available. Patient name and address (including zip code) patient birthdate. Navigate addt/eidt prior authorization form; Acthar gel (corticotropin injection) prior authorization (pa) request form.pdf jun 28, 2023 8:06:12 pm Pcp request for transfer of member. 0632 — pharmacy multiple sources. Navigate community based outpatient prior authorization form; Web use the portal to pay your premium, check your deductible, change your doctor, request an id card and more. Most forms are available in section v of your provider manual. Some of the forms used by arkansas medicaid and its providers are available in electronic format. The patient must have a diagnosis. Page 1 of 1 if the following information is not complete, correct, or legible, the prior authorization (pa) process can be delayed. Not a member?choose a health insurance plan. Some of the forms used by arkansas medicaid and its providers are available in electronic format. Web use the portal to pay your premium, check your deductible, change your doctor, request. Navigate addt/eidt prior authorization form; Confidential and proprietary property of ebrx page 2 of 395 abiraterone (zytiga®) 250 mg tablets. Web ðï ࡱ á> þÿ x | þÿÿÿw. Page 1 of 1 if the following information is not complete, correct, or legible, the prior authorization (pa) process can be delayed. The forms below cannot be printed from this manual for use. Web services billed with the following revenue code(s) always require prior authorization: When prompted, select 0 for other inquiries, then option 3 for provider enrollment. Hospital or ambulatory surgery center name. Patient name and address (including zip code) patient birthdate. Web medicaid, arhome, and arkids beneficiaries watch for your renewal form, fill it out, and return it to arkansas medicaid right away to avoid losing medicaid coverage if you are eligible. Navigate aba prior authorization form; Some of the forms used by arkansas medicaid and its providers are available in electronic format. Official billing forms that are accepted by arkansas medicaid include a barcode and an micr line. Learn more the official website of the state of arkansas The following always require prior authorization: Box 1437, slot s413 p.o. This model of care was developed to address the overall health care needs of medicaid beneficiaries who have complex behavioral health or intellectual and developmental disability (idd) service needs. The patient must have a diagnosis of relapsing. Arkansas medicaid state supplemental rebate contract template. Web arkansas medicaid prior (rx) authorization form.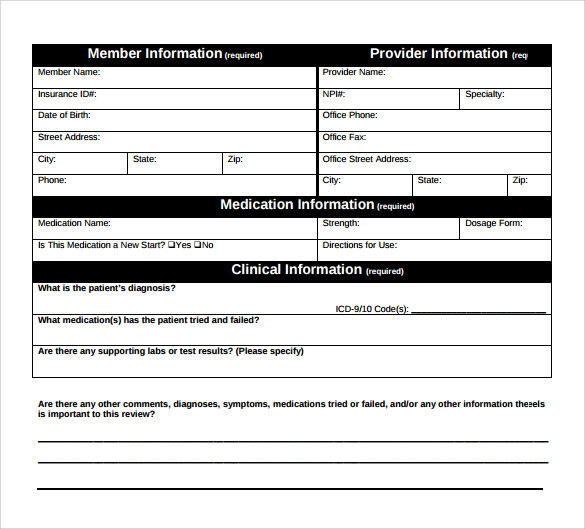
FREE 7+ Medicaid Prior Authorization Forms in PDF
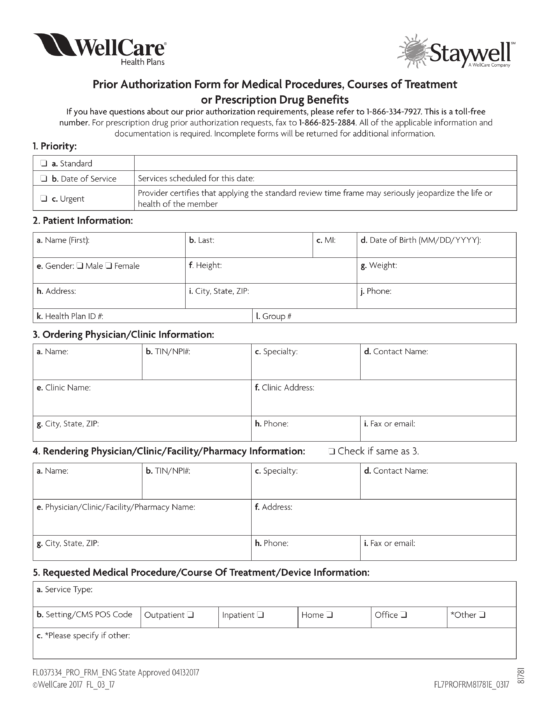
Free WellCare Prior (Rx) Authorization Form PDF eForms
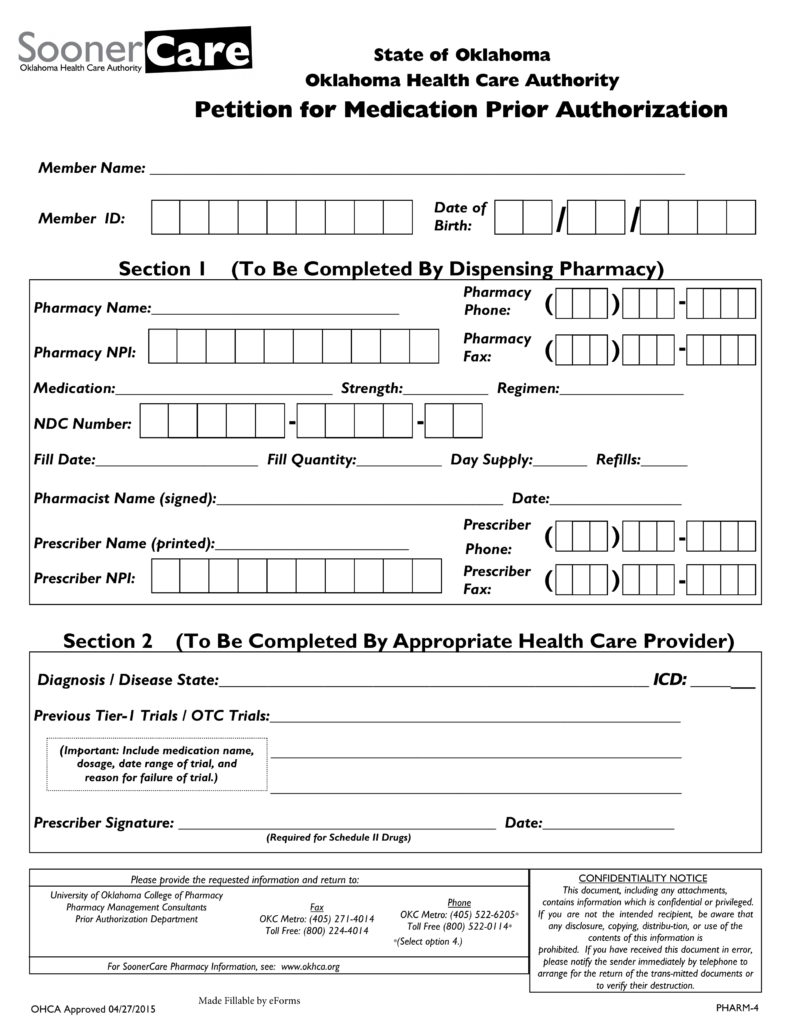
Free Oklahoma Medicaid Prior Authorization Form PDF eForms
Collection Of Prior Authorization Drug List Manulife Free Nude Porn
Prior Authorization Fax Request Form Fill Online, Printable, Fillable

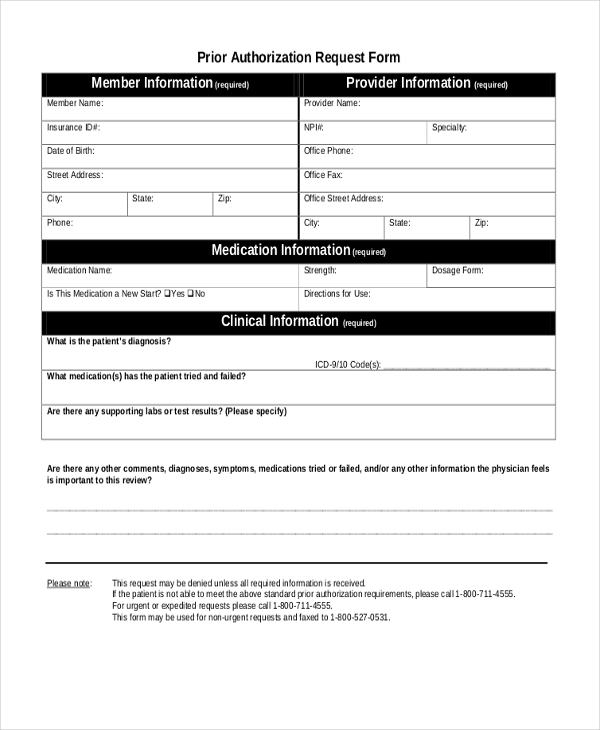
20202023 Form AR Medicaid Prior Authorization RequestFill Online

Free Arkansas Medicaid Prior (Rx) Authorization Form PDF eForms
DMS320 Arkansas Medicaid
Medication Prior Authorization Request Form United Healthcare
OH Medicaid Managed Care Pharmacy Prior Authorization Request Form
Related Post: