Molina Healthcare Appeal Form
Molina Healthcare Appeal Form - Molina healthcare of flor ida appeals & grievance unit po. Web mail this form to: Number of pages (including this cover sheet): Ad molina dispute resolution req & more fillable forms, register and subscribe now! Stop, suspend, reduce or deny a service or; Complaints (appeals) to molina medicare to change a decision about what services we will cover or what we will pay for part 2. Complete this form and mail or fax to: Web molina healthcare member grievance/appeal request form instructions for iling a grievance/appeal: Web if molina medicare or one of our plan providers reduces or cuts back on services or benefits you have been receiving, you can file an appeal. Web provider claims appeal request form provider information: Stop, suspend, reduce or deny a service or; Complaints (appeals) to molina medicare to change a decision about what services we will cover or what we will pay for part 2. Ad molina dispute resolution req & more fillable forms, register and subscribe now! Describe the issue(s) in as much. Web molina healthcare member grievance/appeal request form instructions for iling. Web mail this form to: If you do not agree with molina's choice to deny a requested service (s), and you ask that we change our. Complete this form and mail or fax to: Web dispute resolution request form. Fill out this form completely. Web join the molina healthcare family today. Web filing an appeal or grievance with molina complete care (mcc) there are several ways members or their authorized representative (including a provider on behalf. Web by submitting my information via this form, i consent to having molina healthcare collect my personal information. Web mail this form to: Web how to file an. Complete this form and mail or fax to: Stop, suspend, reduce or deny a service or; Number of pages (including this cover sheet): Web wisconsin provider appeal form line of business: Web filing an appeal or grievance with molina complete care (mcc) there are several ways members or their authorized representative (including a provider on behalf. Web provider claims appeal request form provider information: Web filing an appeal or grievance with molina complete care (mcc) there are several ways members or their authorized representative (including a provider on behalf. Molina healthcare of flor ida appeals & grievance unit po. Web submit the completed form through one of the following: Web quality service > appeals you can. Web by submitting my information via this form, i consent to having molina healthcare collect my personal information. Web an appeal can be filed when you do not agree with molina medicare’s decision to: Web wisconsin provider appeal form line of business: Present your information in person. Complete this form and mail or fax to: Web by submitting my information via this form, i consent to having molina healthcare collect my personal information. Web how to appeal a denial. Number of pages (including this cover sheet): If you think we are. Web cover letter/appeal dispute form containing: Web you may submit the completed form through one of the following ways: Web mail this form to: Present your information in person. Web filing an appeal or grievance with molina complete care (mcc) there are several ways members or their authorized representative (including a provider on behalf. Web how to file an appeal | medicaid an appeal can be. Web if molina medicare or one of our plan providers reduces or cuts back on services or benefits you have been receiving, you can file an appeal. Web filing an appeal or grievance with molina complete care (mcc) there are several ways members or their authorized representative (including a provider on behalf. Web mail this form to: Web how to. Number of pages (including this cover sheet): Web by submitting my information via this form, i consent to having molina healthcare collect my personal information. Complete this form and mail or fax to: Web you may submit the completed form through one of the following ways: Stop, suspend, reduce or deny a service or; If you do not agree with molina's choice to deny a requested service (s), and you ask that we change our. Web an appeal can be filed when you do not agree with molina medicare’s decision to: Web how to appeal a denial. If you think we are. Web mail this form to: Web submit the completed form through one of the following: Describe the issue(s) in as much. Molina healthcare of flor ida appeals & grievance unit po. Web quality service > appeals you can file an appeal what is an appeal? Web molina healthcare member grievance/appeal request form instructions for iling a grievance/appeal: Web wisconsin provider appeal form line of business: Web how to file an appeal | medicaid an appeal can be filed when you do not agree with molina healthcare's decision to stop, suspend, reduce or deny a service or. Stop, suspend, reduce or deny a service or; Web dispute resolution request form. Web if molina medicare or one of our plan providers reduces or cuts back on services or benefits you have been receiving, you can file an appeal. Ad molina dispute resolution req & more fillable forms, register and subscribe now! Fill out this form completely. Web join the molina healthcare family today. Web you may submit the completed form through one of the following ways: Web filing an appeal or grievance with molina complete care (mcc) there are several ways members or their authorized representative (including a provider on behalf.
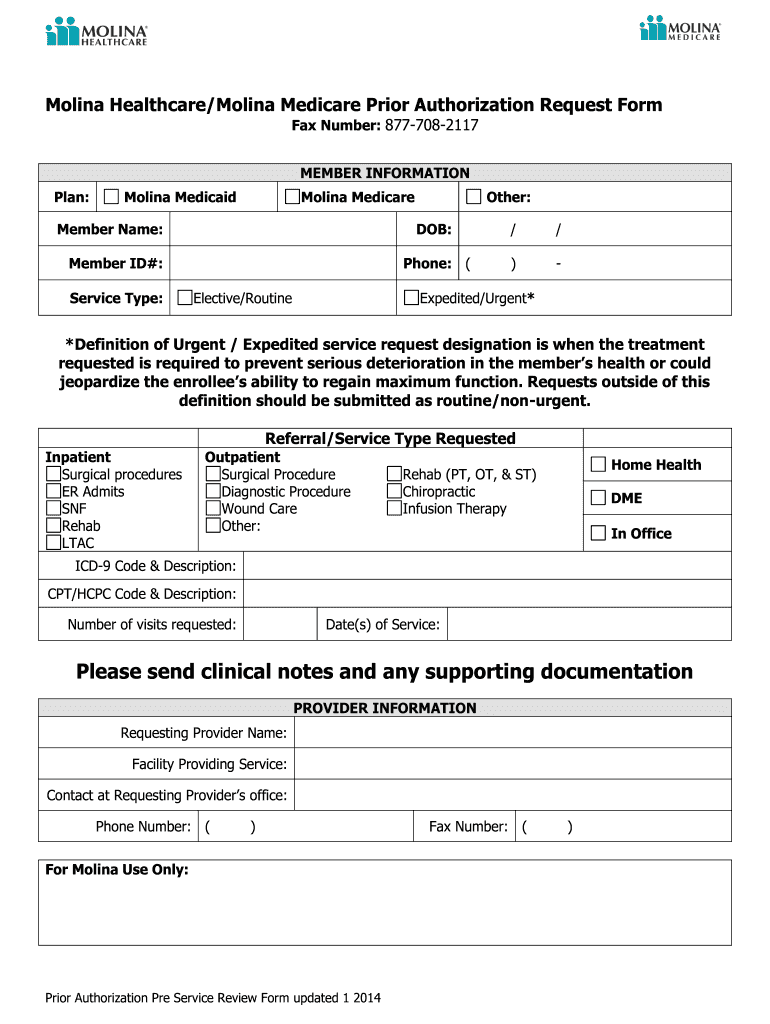
Molina Prior Authorization Request Form Texas Fill Out and Sign
Molina Healthcare Medicaid And Medicare Prior Authorization Request

Molina Healthcare Medication Prior Authorization/Exceptions Request
Molina prior authorization form Fill out & sign online DocHub
Molina provider dispute resolution form Fill out & sign online DocHub
Molina Prior Authorization Form Fill Out and Sign Printable PDF

Molina Medicare Pa Forms Universal Network
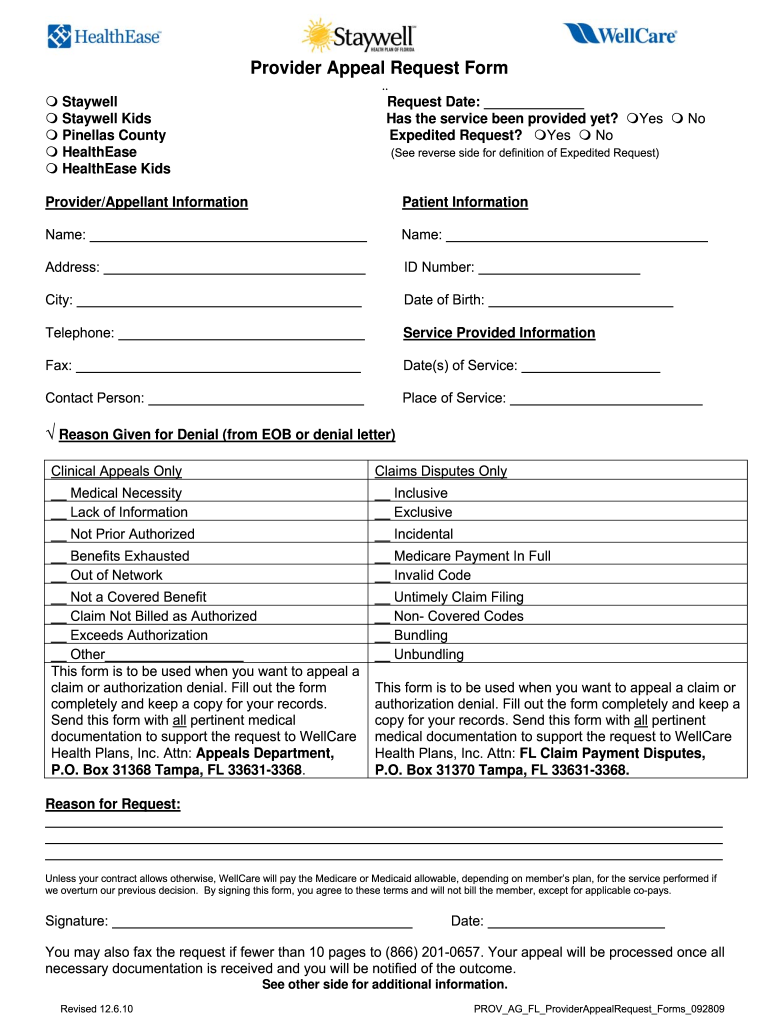
Wellcare Appeal Form Pdf Fill Online, Printable, Fillable, Blank
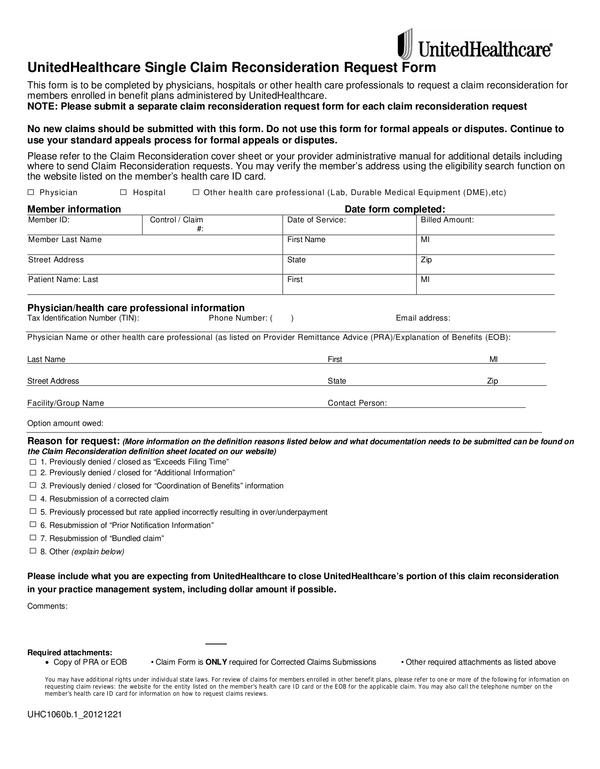
Top United Healthcare Appeal Form Templates Free To Download In PDF

20162023 United HealthCare Background Appeal Form Fill Online
Related Post: