Modivcare Medical Necessity Form
Modivcare Medical Necessity Form - Web modivcare is a transportation coordinating company contracted with the virginia department of medical assistance services (dmas) to manage fee for service (ffs). The modivcare healthcare facility department staff can also fax. Web the following provides access and/or information for many cms forms. Find a plan that saves you money. We provide information and forms organized by state for our facility partners at modivcare. Find gas/mileage reimbursement, level of service, member information sheet, and more forms for your location and needs. Mymodivcare is your transportation provider for reliable, personalized care. Web the purpose of this form is for physicians to communicate to modivcaretm (formerly logisticare) specific transportation restrictions of a patient/member due to a medical. Required for all patients / members using wheelchair or stretcher transport. Web medical necessity form is needed for any member who requires stretcher level of service. Bring essential care right to you. Web the following provides access and/or information for many cms forms. Web the purpose of this form is for physicians to communicate to modivcaretm specific transportation restrictions of a patient/member due to a medical condition. Web •physician or nurse must complete medical necessity form. ( ) patient name (last, first, mi) medicaid provider name. Web •physician or nurse must complete medical necessity form. Web a certificate of medical necessity (cmn) or a dme information form (dif) is a form required to help document the medical necessity and other coverage criteria. Web this form should be completed by the attending physician or his staff to confirm medical necessity of rider not being able to use. Web this form should be completed by the attending physician or his staff to confirm medical necessity of rider not being able to use public transportation. Web modivcare is a transportation coordinating company contracted with the virginia department of medical assistance services (dmas) to manage fee for service (ffs). The medical necessity form should accompany a standing. Ad compare all. The medical necessity form should accompany a standing. The medical necessity form should. Web medical necessity form to be completed by medical provider (md, rn, pa, np) medical director po box 11647 new brunswick, nj 08906 phone: Web •physician or nurse must complete medical necessity form. ( ) patient name (last, first, mi) medicaid provider name & address. Web a copy of the medical necessity form is located at this web site and can be downloaded for your convenience. Bring essential care right to you. The medical necessity form should accompany a standing. Web the purpose of this form is for physicians to communicate to modivcaretm specific transportation restrictions of a patient/member due to a medical condition. Web. The modivcare healthcare facility department staff can also fax. We provide information and forms organized by state for our facility partners at modivcare. The medical necessity form should accompany a standing. Required for all patients / members using wheelchair or stretcher transport. Web the following provides access and/or information for many cms forms. Web this form should be completed by the attending physician or his staff to confirm medical necessity of rider not being able to use public transportation. Web a copy of the medical necessity form is located at this web site and can be downloaded for your convenience. Web medical necessity form is needed for any member who requires stretcher level. Web •physician or nurse must complete medical necessity form. Please click on the title that corresponds to the document you would like to view. The medical necessity form should accompany a standing. Web the purpose of this form is for physicians to communicate to modivcaretm (formerly logisticare) specific transportation restrictions of a patient/member due to a medical. The medical necessity. Bring essential care right to you. Web this form should be completed by the attending physician or his staff to confirm medical necessity of rider not being able to use public transportation. You may also use the search feature to more quickly locate information for a specific form. Web the following provides access and/or information for many cms forms. Web. Bring essential care right to you. Web medical necessity form to be completed by medical provider (md, rn, pa, np) medical director po box 11647 new brunswick, nj 08906 phone: ( ) patient name (last, first, mi) medicaid provider name & address. Web •physician or nurse must complete medical necessity form. Ad compare all your options at medicare.gov, the official. Bring essential care right to you. The medical necessity form should. The medical necessity form should accompany a standing. Ad compare all your options at medicare.gov, the official source for medicare information. Please click on the title that corresponds to the document you would like to view. Web a copy of the medical necessity form is located at this web site and can be downloaded for your convenience. Web a copy of the medical necessity form is located at this web site and can be downloaded for your convenience. Web the purpose of this form is for physicians to communicate to modivcaretm specific transportation restrictions of a patient/member due to a medical condition. The modivcare healthcare facility department staff can also fax. Web an attending physician, physician assistant, nurse practitioner, clinical nurse specialist or rn can complete the medical necessity form. Web this form should be completed by the attending physician or his staff to confirm medical necessity of rider not being able to use public transportation. Web medical provider level of service certification fax: Web medical necessity form is needed for any member who requires stretcher level of service. You may also use the search feature to more quickly locate information for a specific form. Web •physician or nurse must complete medical necessity form. The modivcare healthcare facility department staff can also fax. It pays to compare rx and health coverage options. Required for all patients / members using wheelchair or stretcher transport. We provide information and forms organized by state for our facility partners at modivcare. Web this form should be completed by the attending physician or his staff to confirm medical necessity of rider not being able to use public transportation.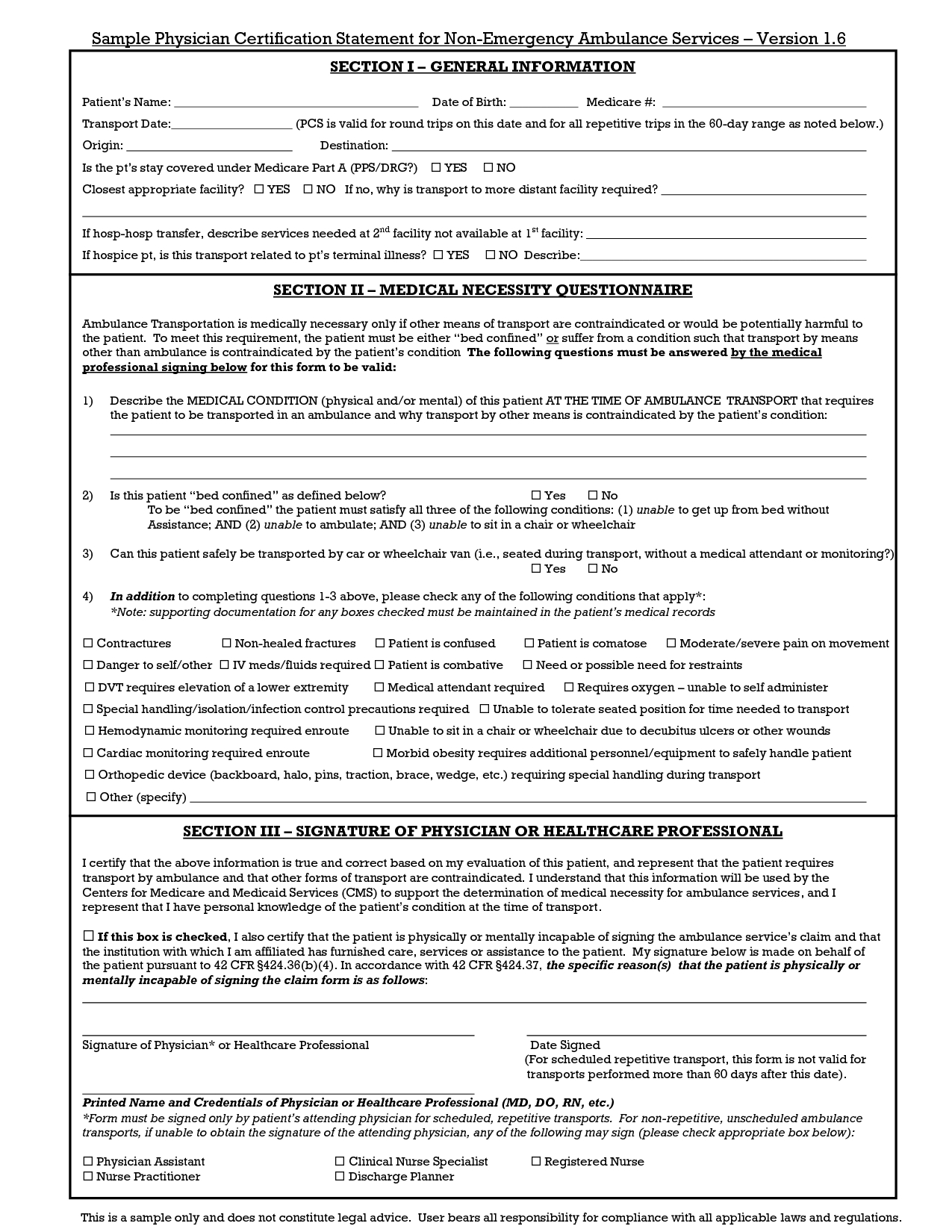
Letter Of Medical Necessity Fsa Template Samples Letter Template
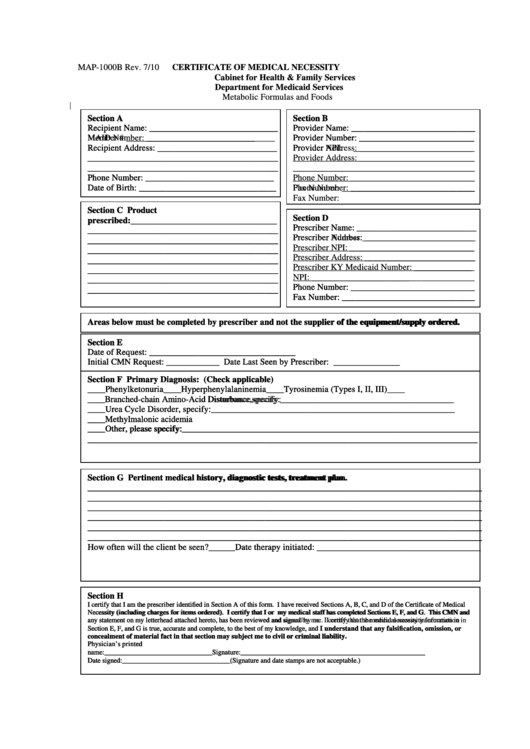
Top 6 Medicare Medical Necessity Form Templates free to download in PDF
Doctor Letter Of Medical Necessity Template
Medically Necessary Sample Letter Of Medical Necessity Template
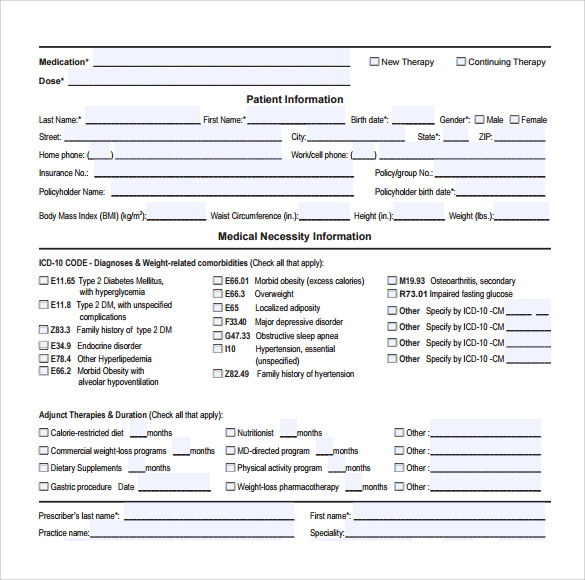
Medical Necessity Form templates free printable
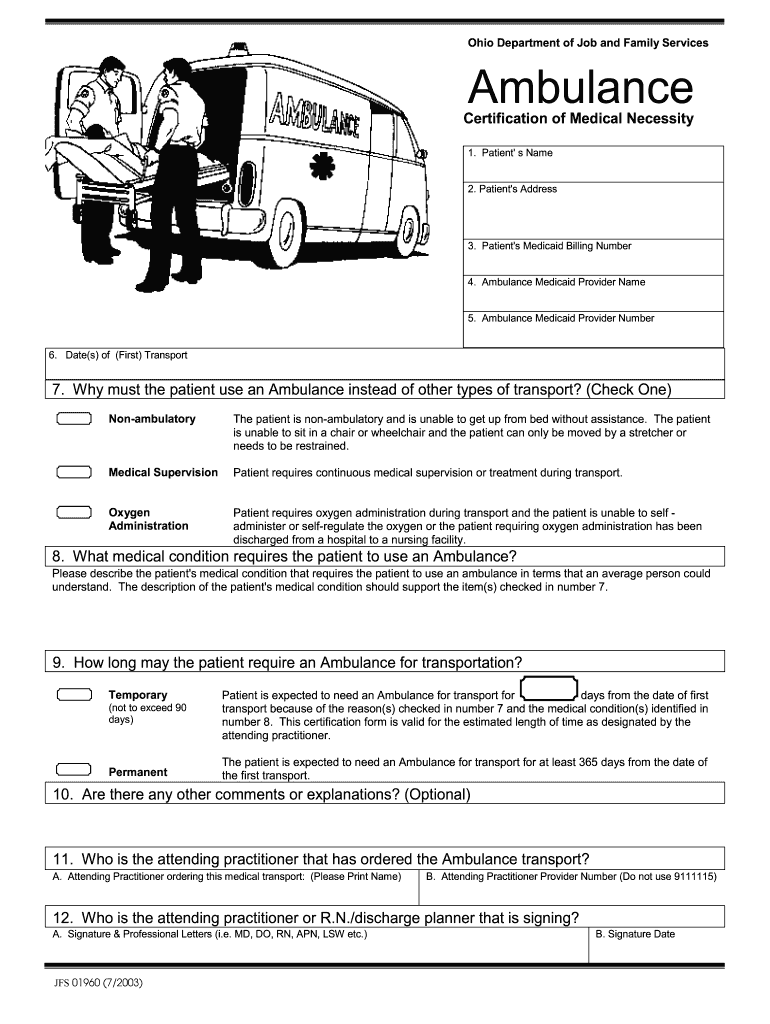
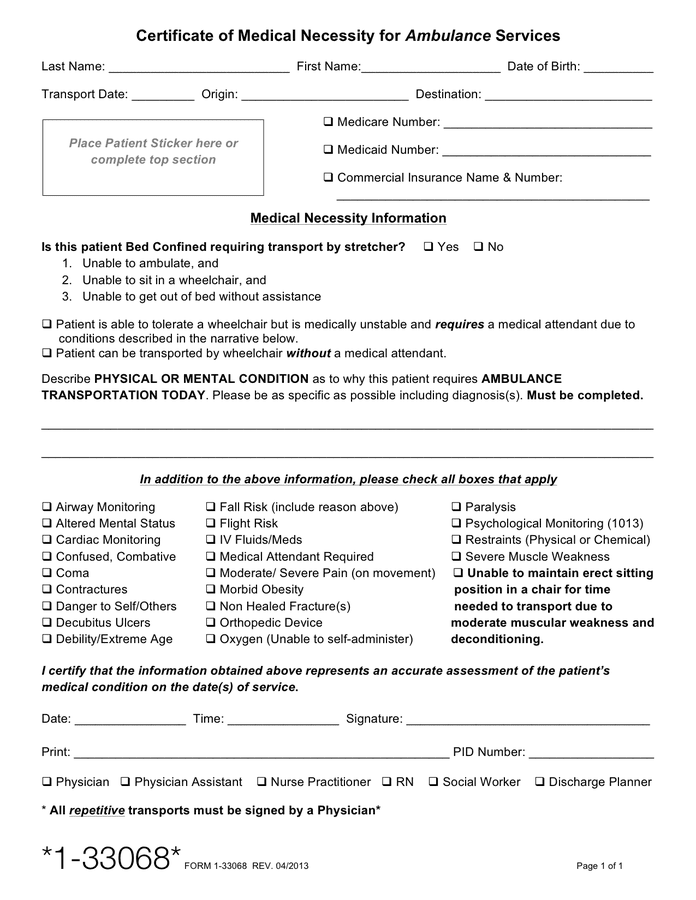
Ambulance Medical Necessity Form Fill Out and Sign Printable PDF
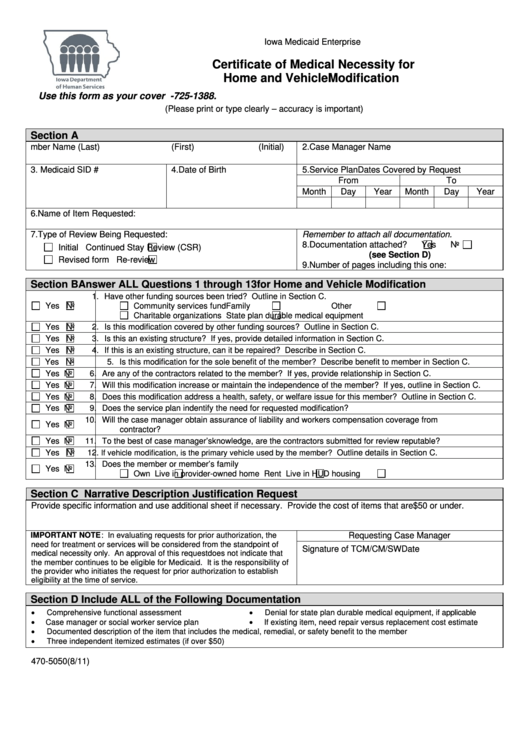
Certificate Of Medical Necessity For Home And Vehicle Modification
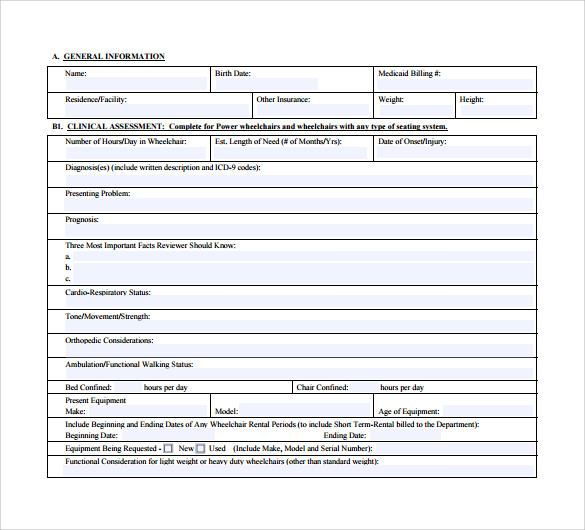
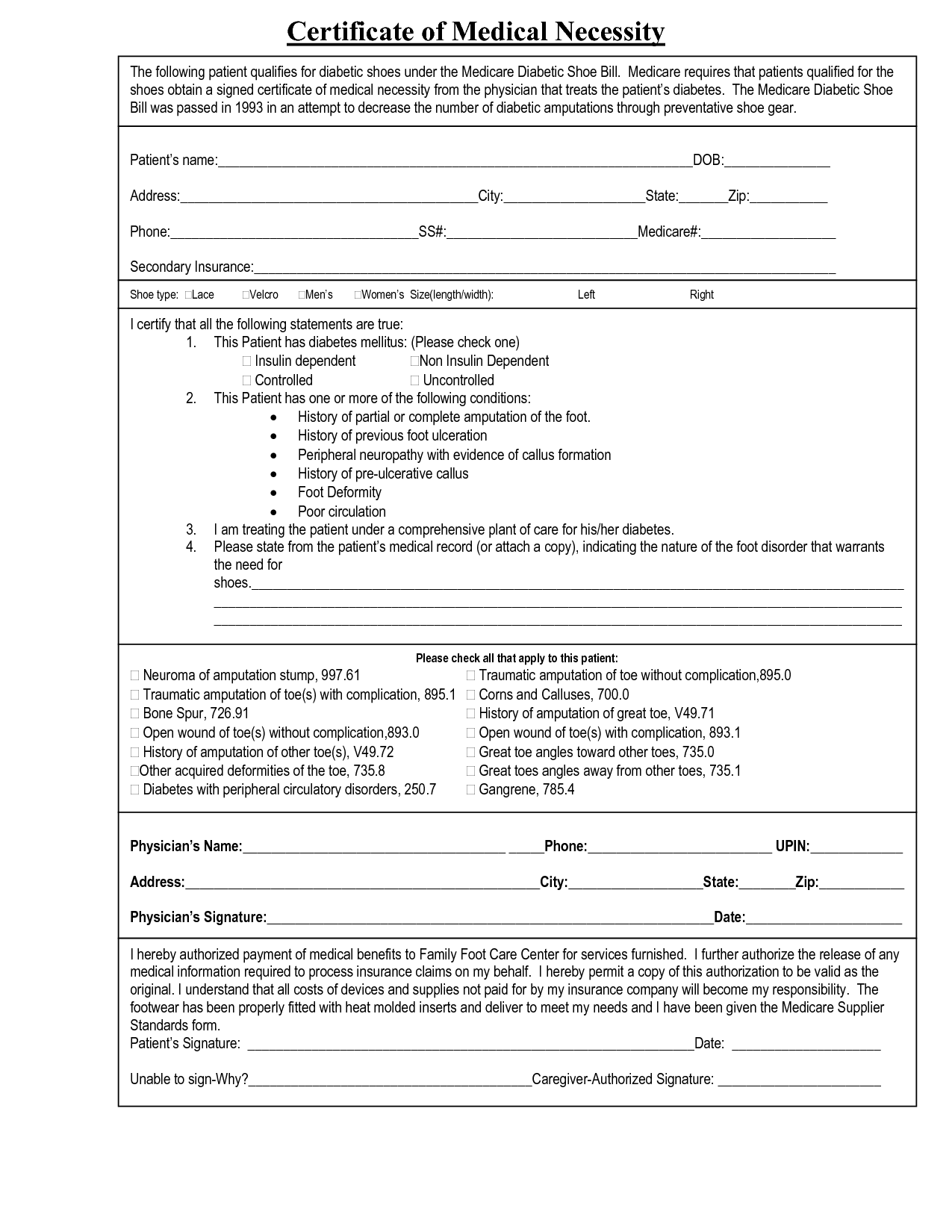
Certificate Of Medical Necessity Form Template
Sample Letter Of Medical Necessity For Panniculectomy Fill Online

Omnipod Necessity Form Fill Out and Sign Printable PDF Template signNow
Related Post: