Kevzara Enrollment Form
Kevzara Enrollment Form - People with medicare who want to join a medicare advantage. If you are applying for financial. Web patient consent and enrollment form instructions to ensure your information is processed without delay: If you have patients who may meet eligibility requirements and would like to enroll in the program, download and complete the form below and fax page 1 to. Ad learn more about kevzara here. Ad learn more about kevzara here. Patient information and prescription insurance cards. Easily fill out pdf blank, edit, and sign them. You'll find more details at www.kevzara.com. 08/2019 learn about the personalized services. They’ll then adjust your dosage if your blood tests indicate it needs to be changed. View boxed warning, prescribing & safety info. Service benefit plan prior approval p.o. Talk to your doctor about an oral pill for rheumatoid arthritis. If you are applying for financial. People with medicare who want to join a medicare advantage. View boxed warning, prescribing & safety info. You'll find more details at www.kevzara.com. Patient information and prescription insurance cards. 11/16/2021 send completed form to: Ad kevzara® prescription treatment— view boxed warning & safety info. Web agents (together , the “alliance”) to provide me services under the program, as described in this program enrollment form and as may be added in the future. Complete section 1 sign section 2 3. Web prescription & enrollment form kevzara® (sarilumab) for pmr four simple steps to submit your. Ad learn more about kevzara here. If you have patients who may meet eligibility requirements and would like to enroll in the program, download and complete the form below and fax page 1 to. Web prescription & enrollment form kevzara® (sarilumab) for pmr four simple steps to submit your referral. 11/16/2021 send completed form to: Web the dosage of kevzara. View terms and conditions and privacy. Web patient consent and enrollment form instructions to ensure your information is processed without delay: If you are applying for financial. View boxed warning, prescribing & safety info. Ad discover an ra treatment option that can help stop irreversible joint damage & stiffness. View boxed warning, prescribing & safety info. 11/16/2021 send completed form to: Web patient consent and enrollment form instructions to ensure your information is processed without delay: Patient information and prescription insurance cards. Web by submitting this form, i certify that i am at least 18 years old and agree to receive information and resources about kevzara. If you have patients who may meet eligibility requirements and would like to enroll in the program, download and complete the form below and fax page 1 to. Complete section 1 sign section 2 3. 11/16/2021 send completed form to: 08/2019 learn about the personalized services. Patient information and prescription insurance cards. 11/16/2021 send completed form to: If you have patients who may meet eligibility requirements and would like to enroll in the program, download and complete the form below and fax page 1 to. Web patient consent and enrollment form instructions to ensure your information is processed without delay: Talk to your doctor about an oral pill for rheumatoid arthritis. Save. Kevzara 200mg prefilled syringe kevzara 150mg prefilled. Web kevzara® (sarilumab) is indicated for treatment of adult patients with moderately to severely active rheumatoid arthritis (ra) who had an inadequate response or intolerance. Ad kevzara® prescription treatment— view boxed warning & safety info. Web agents (together , the “alliance”) to provide me services under the program, as described in this program. All information will be kept confidential and will not. Complete section 1 sign section 2 3. Use get form or simply click on the template preview to open it in the editor. If you are applying for financial. Ad learn more about kevzara here. Web this form are completed.** specialty: Web the dosage of kevzara for ra is 200 mg once every 2 weeks. Service benefit plan prior approval p.o. Northern california or southern california region individual plan who can use this form? If you are applying for financial. View boxed warning, prescribing & safety info. If you have patients who may meet eligibility requirements and would like to enroll in the program, download and complete the form below and fax page 1 to. Ad kevzara® prescription treatment— view boxed warning & safety info. They’ll then adjust your dosage if your blood tests indicate it needs to be changed. Talk to your doctor about an oral pill for rheumatoid arthritis. Easily fill out pdf blank, edit, and sign them. View boxed warning, prescribing & safety info. All information will be kept confidential and will not. Kevzara 200mg prefilled syringe kevzara 150mg prefilled. 08/2019 learn about the personalized services. Ad learn more about kevzara here. You'll find more details at www.kevzara.com. Complete section 1 sign section 2 3. Web prescription & enrollment form kevzara® (sarilumab) for pmr four simple steps to submit your referral. Web by submitting this form, i certify that i am at least 18 years old and agree to receive information and resources about kevzara.
Sanofi and Regeneron Announce FDA Approval of Kevzara® (sarilumab) for
RSBSA Enrollment Form PDF Farms Livestock

Enrollment Form Template Word DocTemplates

Greenville County Schools Enrollment Forms Enrollment Form

KEVZARA® 150 mg 6 St

DepEd Basic Education Enrollment Form TeacherPH
Kevzara FDA prescribing information, side effects and uses
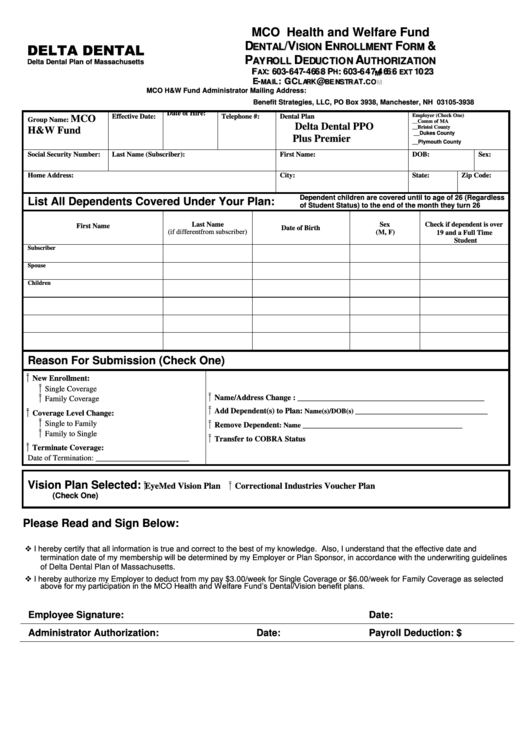
Enrollment Form Benefit Strategies printable pdf download

Sarilumab Sarilumab Abmole Bioscience Sarilumab Price Learn how to

These highlights do not include all the information needed to use
Related Post:
