Kaiser Provider Appeal Form California
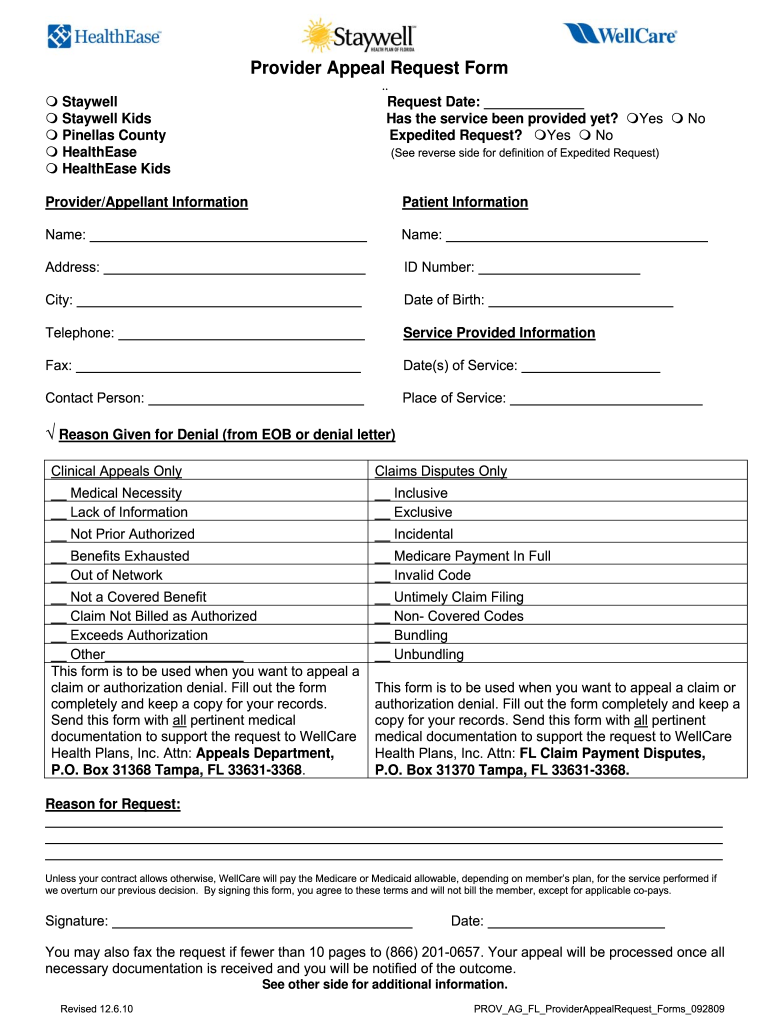
Kaiser Provider Appeal Form California - Easily sign the kaiser permanente appeal form with your finger. Web either writing to kaiser permanente, special services unit, p.o. Y0043_ n00016915_c this document and others if attached contain information that is. Kaiser permanente follows state and federal civil rights laws. Web if awarded, the program will cover emergency or medically necessary care from kaiser permanente providers or at kaiser permanente facilities for a specified time period. * if the denial document states the payment is the provider’s responsibility, then the provider must submit a. Timely submission of provider request for. Resubmission or reconsideration on the claim form. National claims administration 1800 harrison street, 8th. If you have any questions or need help with your application,. Be a qualified, immediate family member living in the same home as a current kaiser permanente member. If you have any questions or need help with your application,. Web discrimination is against the law. Send your completed and signed form to: Resubmission or reconsideration on the claim form. Web kaiser permanente has also pledged to make additional significant investments, totaling $150 million over 5 years, into programs to improve the delivery of. Kaiser foundation health plan, inc. To do this, you should provide the. Web health care information form signed by the member. Web if awarded, the program will cover emergency or medically necessary care from kaiser permanente. Be a qualified, immediate family member living in the same home as a current kaiser permanente member. Web you may submit your provider dispute notice on our provider dispute resolution request form (pdrr) (attached). Web discrimination is against the law. Web kaiser permanente has also pledged to make additional significant investments, totaling $150 million over 5 years, into programs to. Patient's name, date of birth, and member id number 2. Northern california or southern california region individual plan. Send your completed and signed form to: Reason for denial, member name, medical record number, service dates and. Web you may submit your provider dispute notice on our provider dispute resolution request form (pdrr) (attached). Send filled & signed kaiser appeal. Reason for denial, member name, medical record number, service dates and. Be a qualified, immediate family member living in the same home as a current kaiser permanente member. Patient's name, date of birth, and member id number 2. Web appeal is submitted without appeal filing form, the information listed below must be present: Web you may also file an appeal if your medical expenses exceed 10% of your annual gross household income over the previous 12 months. If you have questions about these requirements or medicaid. Kaiser foundation health plan, inc., in northern and southern. Web complete this form to attest that your company continues to meet the minimum participation and contribution requirements. If you have any questions or need help with your application,. Kaiser permanente follows state and federal civil rights laws. Web you may also file an appeal if your medical expenses exceed 10% of your annual gross household income over the previous 12 months. Resubmission or reconsideration on the claim form. Contracted providers have 24 months from the notification date. Reason for denial, member name, medical record number, service dates and. Box 1809 pleasanton ca 94566. Timely submission of provider request for. Easily sign the kaiser permanente appeal form with your finger. Web health care information form signed by the member. For your claim to be considered for payment, follow these simple steps: Box 1809 pleasanton ca 94566. National claims administration 1800 harrison street, 8th. Web northern california medicare provider directory (tagalog) (updated 01/27/23) (pdf) northern california medicare provider directory (vietnamese) (updated 01/27/23) (pdf). Northern california or southern california region individual plan. Send filled & signed kaiser appeal. For your claim to be considered for payment, follow these simple steps: Contracted providers have 24 months from the notification date of denial. Be a qualified, immediate family member living in the same home as a current kaiser permanente member. National claims administration 1800 harrison street, 8th. Y0043_ n00016915_c this document and others if attached contain information that is. Send your completed and signed form to: Open the kaiser provider dispute form and follow the instructions. Box 1809 pleasanton ca 94566. Web northern california medicare provider directory (tagalog) (updated 01/27/23) (pdf) northern california medicare provider directory (vietnamese) (updated 01/27/23) (pdf). Web health care information form signed by the member. Easily sign the kaiser permanente appeal form with your finger. * if the denial document states the payment is the provider’s responsibility, then the provider must submit a. Web up to $40 cash back the information that must be reported on a kaiser provider appeal form includes: Be a qualified, immediate family member living in the same home as a current kaiser permanente member. Kaiser permanente insurance company member relations appeals p.o. For groups with 20+ eligible employees, use the federal cobra application to cover your client’s former employees and their dependents. Web what is the timely filing limit for kaiser california appeal? Web to appeal the decision, please send your request for review to: Contracted providers have 24 months from the notification date of denial. Web kaiser permanente has also pledged to make additional significant investments, totaling $150 million over 5 years, into programs to improve the delivery of. Kaiser permanente does not unlawfully discriminate, exclude people, or treat them. To do this, you should provide the. Web appeal is submitted without appeal filing form, the information listed below must be present: For your claim to be considered for payment, follow these simple steps:
2015 Form CA Kaiser NS9934 Fill Online, Printable, Fillable, Blank
20152020 Form CA Kaiser NS9934 Fill Online, Printable, Fillable
Molina provider dispute resolution form Fill out & sign online DocHub

2016 CA OSHAB Appeal Form 100 Fill Online, Printable, Fillable, Blank
Kaiser Permanente Forms Medical Release Forms Fill Out and Sign
kaiser permanente appeal form Yanira Braswell
California Kaiser Permanente Authorization Form Fill Out and Sign

MERCYCARE PROVIDER APPEAL Doc Template pdfFiller

cigna appeal form Fill out & sign online DocHub
Wellcare Appeal Form Pdf Fill Online, Printable, Fillable, Blank
Related Post: