Ihss Recipient Application Form
Ihss Recipient Application Form - Web registration register for the ihss website to: Web the original form and give you a copy. You must physically reside in the united states. You must also be a california resident. Web find the ihss application form pdf you require. Applicant/recipient information (to be completed by the county) applicant/recipient name: Web submitting the initial ihss application involves three main components. All sections of this form must be completed. Web submit this form within ten (10) calendar days from the “notice date” listed on the upper right corner of page 1. Second, submit the application and all relevant. Web how to apply for ihss. All sections of this form must be completed. You must also be a california resident. Eligibility criteria for all ihss applicants and recipients: Web find the ihss application form pdf you require. Web please review the provider notice and request form below for additional information. Web submit this form within ten (10) calendar days from the “notice date” listed on the upper right corner of page 1. Web submitting the initial ihss application involves three main components. Web if you want to become an ihss provider, you must complete all the steps. Eligibility criteria for all ihss applicants and recipients: You must also be a california resident. Web the following “commonly used recipient and provider state forms” is available on the california department of social services website at:. Web please review the provider notice and request form below for additional information. Fill in the empty fields; Ask a licensed medical professional to verify your need for ihss by filling out form soc 873. Engaged parties names, places of residence. Web how to apply for ihss. Web registration register for the ihss website to: You may submit this form by mail or in person to your ihss. Information provided is subject to verification. Web find the ihss application form pdf you require. Web submitting the initial ihss application involves three main components. Information provided is subject to veriication. Eligibility criteria for all ihss applicants and recipients: Web they operate a provider registry and will provide you with referrals to providers. Web submitting the initial ihss application involves three main components. Free, fast, full version (2023) available! Second, submit the application and all relevant. All sections of this form must be completed. Web the personal care services program (pcsp) began in april 1993, and was the first ihss program to obtain federal funding for recipients. Web submit the health care certification form soc 873. You may submit this form by mail or in person to your ihss. Web if you want to become an ihss provider, you must complete all the steps. Web submit this form within ten (10) calendar days from the “notice date” listed on the upper right corner of page 1. Eligibility criteria for all ihss applicants and recipients: All sections of this form must be completed. Web the following “commonly used recipient and provider state forms” is available on the california department of social services website at:. Web submitting. Web the recipient who wishes to hire you as his/her provider (or his/her authorized representative) must submit an ihss recipient request for provider waiver (soc 862). All sections of this form must be completed. You must physically reside in the united states. Second, submit the application and all relevant. Web the following “commonly used recipient and provider state forms” is. Web registration register for the ihss website to: Fill in the empty fields; Web if you want to become an ihss provider, you must complete all the steps outlined in the document linked below before you can be enrolled as a provider and receive payment. All sections of this form must be completed. To apply for ihss call: Web submit this form within ten (10) calendar days from the “notice date” listed on the upper right corner of page 1. Engaged parties names, places of residence. Eligibility criteria for all ihss applicants and recipients: Information provided is subject to veriication. Pcsp recipients are eligible for full. Web the original form and give you a copy. You must physically reside in the united states. Ask a licensed medical professional to verify your need for ihss by filling out form soc 873. Web how to apply for ihss. Web the recipient who wishes to hire you as his/her provider (or his/her authorized representative) must submit an ihss recipient request for provider waiver (soc 862). Ad immediate hire ihss apply may be available! Applicant/recipient information (to be completed by the county) applicant/recipient name: View your timesheet and payment statuses enter and submit timesheets no longer mail paper timesheets request additional. Web they operate a provider registry and will provide you with referrals to providers. You may submit this form by mail or in person to your ihss. Web submit the health care certification form soc 873. Web please review the provider notice and request form below for additional information. Web if you want to become an ihss provider, you must complete all the steps outlined in the document linked below before you can be enrolled as a provider and receive payment. Fill in the empty fields; Second, submit the application and all relevant.
Top 17 Ihss Forms And Templates free to download in PDF format

Form SOC873 Download Fillable PDF or Fill Online Inhome Supportive
Ihss Application Form Fill Online, Printable, Fillable, Blank pdfFiller
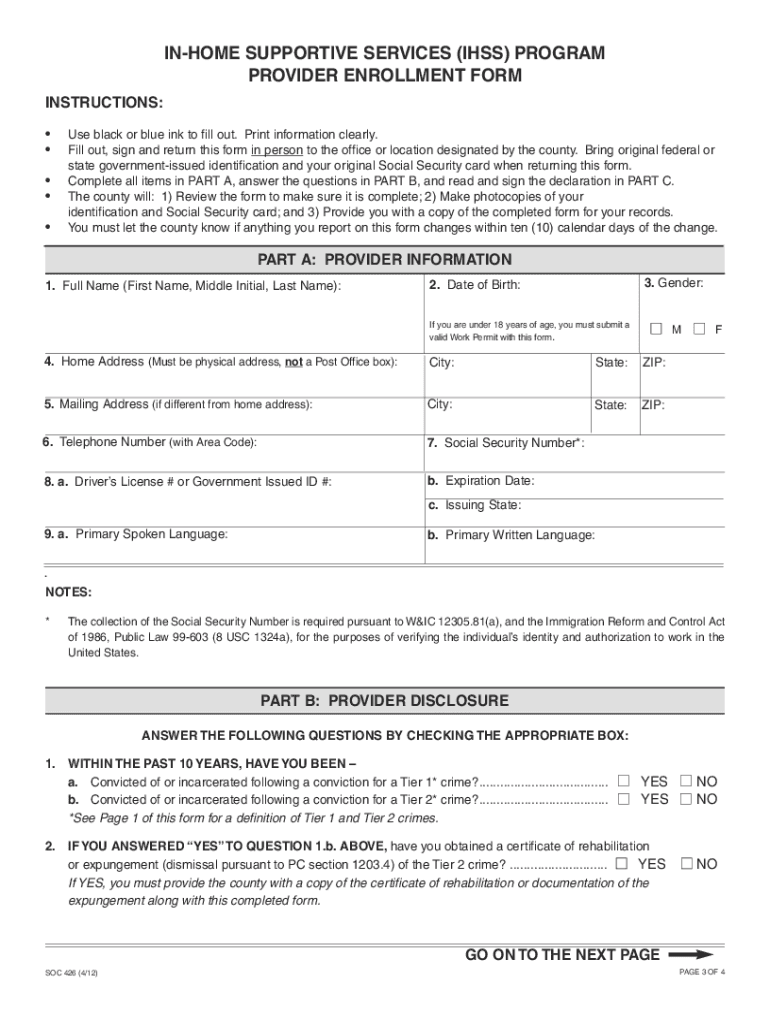
Form SOC426A Download Fillable PDF or Fill Online Inhome Supportive
Fillable Form IhssE 007 InHome Supportive Services (Ihss) Program

Form Soc 2274 InHome Supportive Services (Ihss ) Program
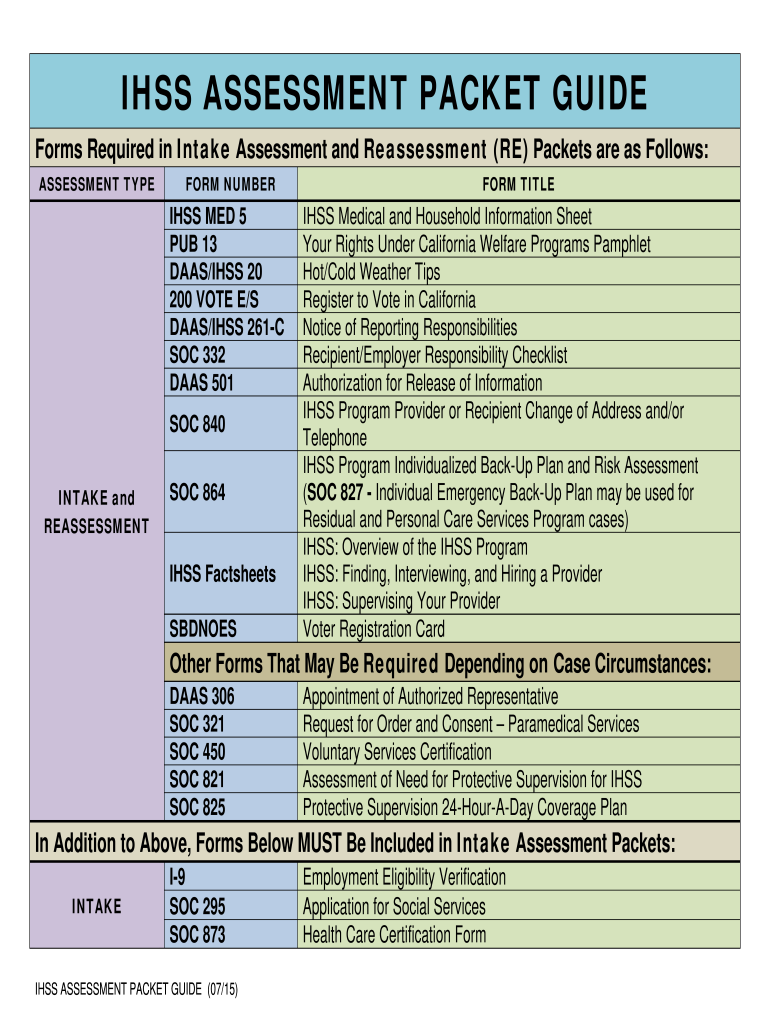
IHSS ASSESSMENT PACKET GUIDE Fill and Sign Printable Template Online
Ihss Application Form Fill Out and Sign Printable PDF Template signNow
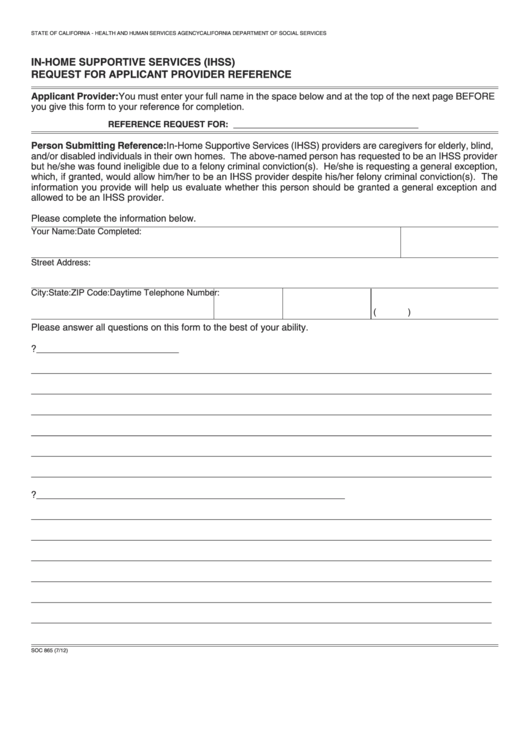
Fillable Form Soc 865 InHome Supportive Services (Ihss) Request For
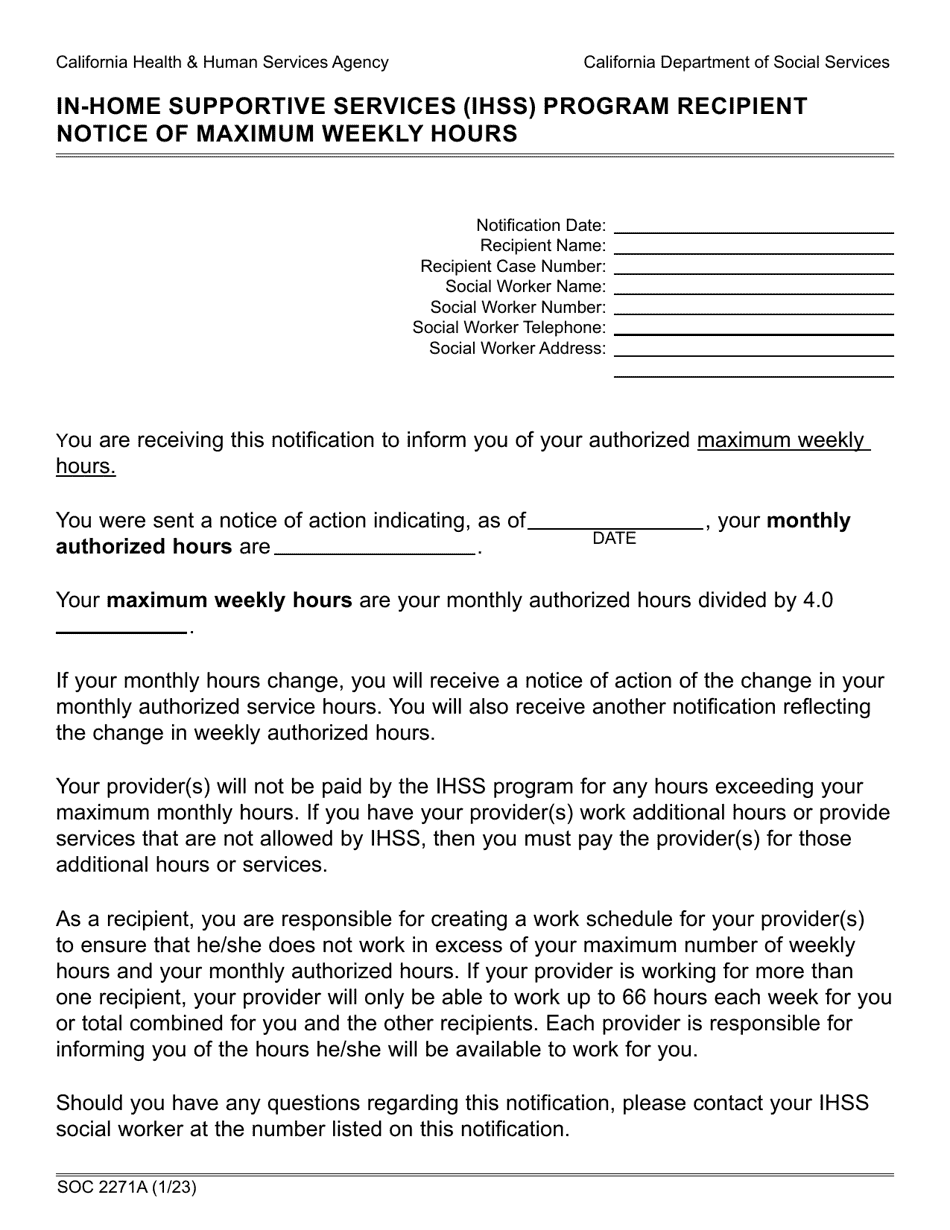
Form SOC2271A Download Fillable PDF or Fill Online Inhome Supportive
Related Post: