Ihss Authorized Representative Form
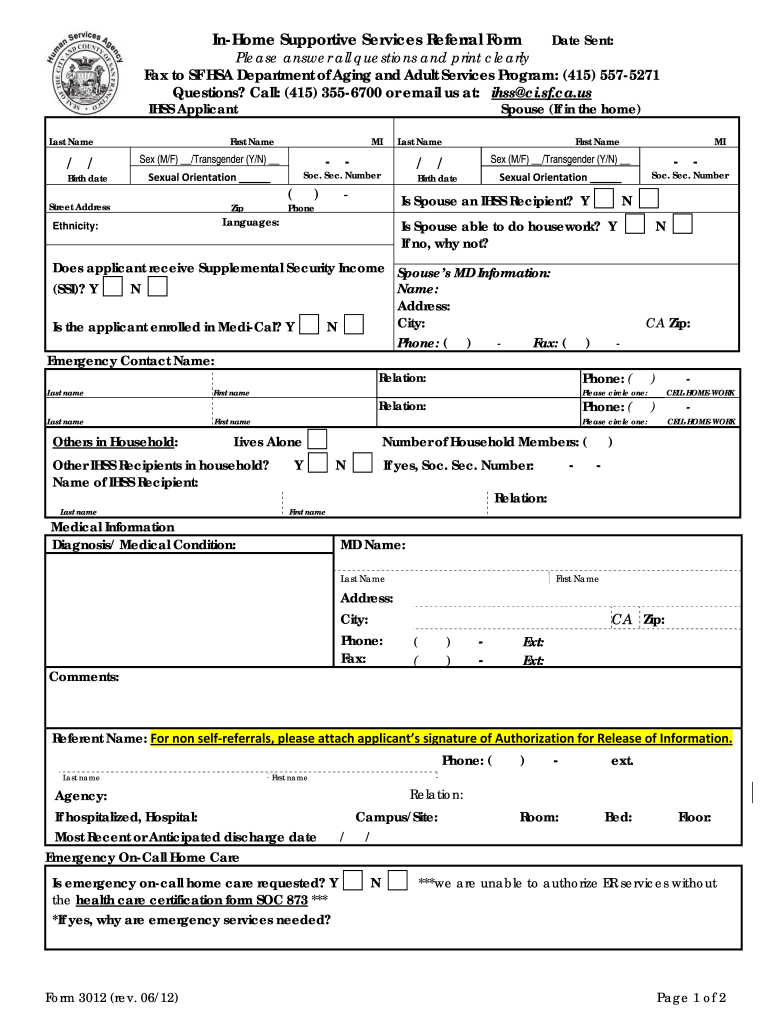
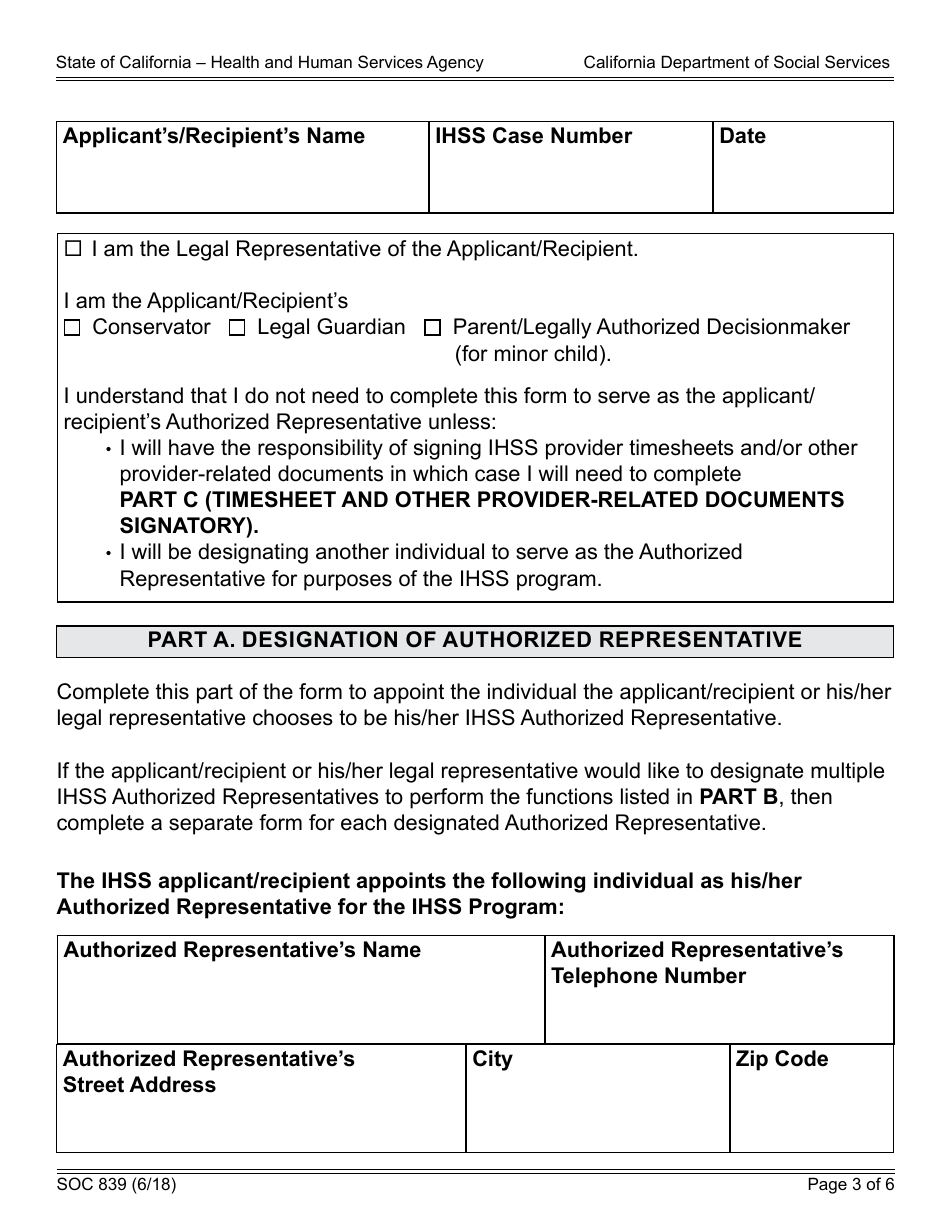
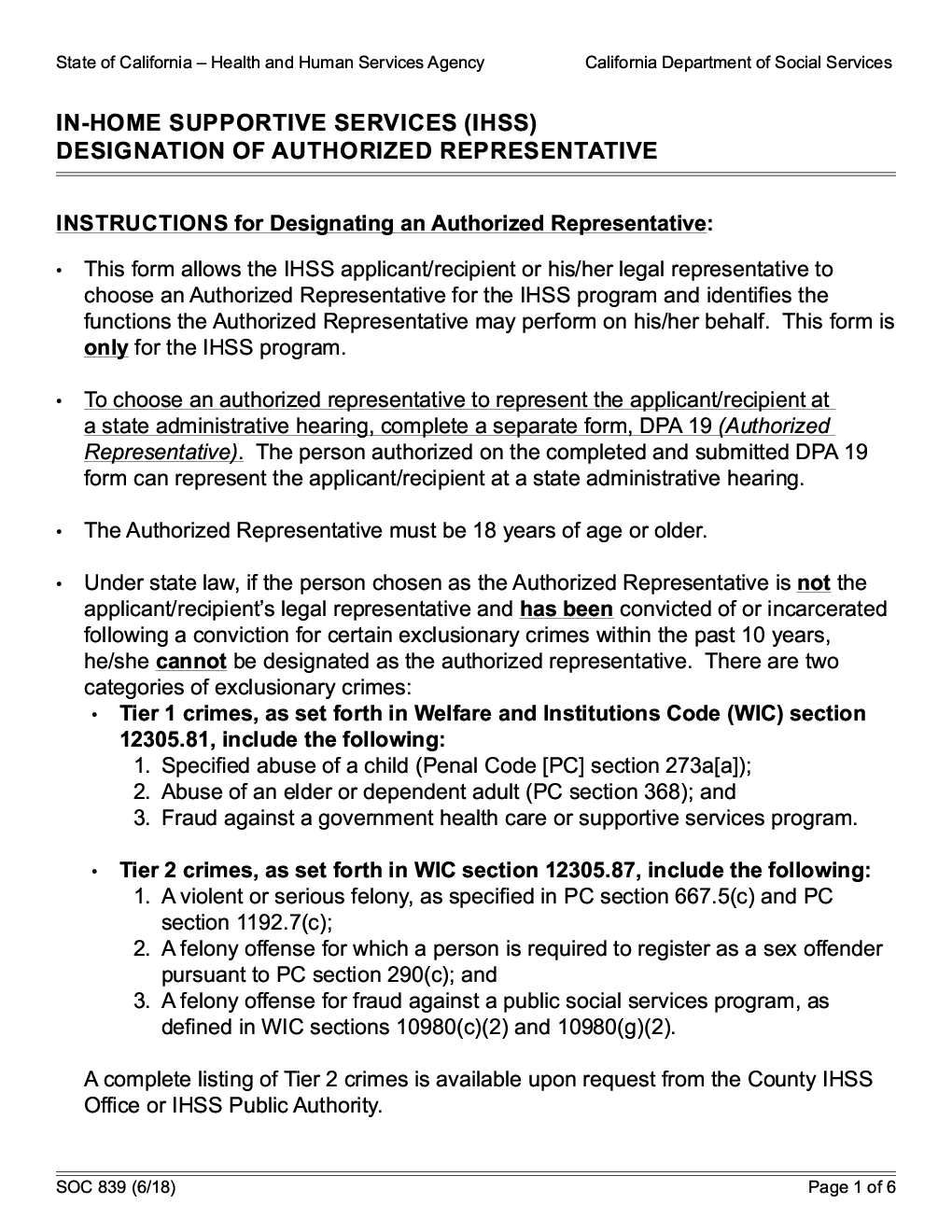
Ihss Authorized Representative Form - A provider is one who is providing services to an ihss recipient in their home. Submit your appeal request form. Web the ihss worker has the responsibility for authorizing services and service hours. Web • you (or your authorized representative) must complete part a of this form to let the county know who you have chosen to provide your authorized services. Web • complete a provider enrollment form and bring in original identity documentation and original social security card • complete and pass a doj criminal background check •. Web sign or have your authorized representative sign, indicate who signed and date your appeal request form. Web authorized representative means an individual designated by the eligible person receiving services, or by the parent or guardian receiving services, if appropriate, who has the. The following are riverside county’s “commonly used ihss forms”. The information provided in this form will be considered as one factor of the need for. Web complete an authorized representative form found at: Web complete an authorized representative form found at: Web sign or have your authorized representative sign, indicate who signed and date your appeal request form. Web authorized representative means an individual designated by the eligible person receiving services, or by the parent or guardian receiving services, if appropriate, who has the. Web • you (or your authorized representative) must complete. Web authorized representative means an individual designated by the eligible person receiving services, or by the parent or guardian receiving services, if appropriate, who has the. Web this document may only be signed by the recipient or by an authorized representative. The following are riverside county’s “commonly used ihss forms”. You may submitthis form by mail or in person to. Web this document may only be signed by the recipient or by an authorized representative. Web the ihss worker has the responsibility for authorizing services and service hours. A provider is one who is providing services to an ihss recipient in their home. Web complete an authorized representative form found at: Web • complete a provider enrollment form and bring. Web the recipient who wishes to hire you as his/her provider (or his/her authorized representative) must submit an ihss recipient request for provider waiver (soc. Web • complete a provider enrollment form and bring in original identity documentation and original social security card • complete and pass a doj criminal background check •. Web authorized representative means an individual designated. Web • complete a provider enrollment form and bring in original identity documentation and original social security card • complete and pass a doj criminal background check •. Submit your appeal request form. You may submitthis form by mail or in person to your ihss county, public authority, or. Submit your appeal request form. Web authorized representative means an individual. The following are riverside county’s “commonly used ihss forms”. Web this document may only be signed by the recipient or by an authorized representative. A provider is one who is providing services to an ihss recipient in their home. Web sign or have your authorized representative sign, indicate who signed and date your appeal request form. Web • you (or. Submit your appeal request form. You may submitthis form by mail or in person to your ihss county, public authority, or. Web authorized representative means an individual designated by the eligible person receiving services, or by the parent or guardian receiving services, if appropriate, who has the. Web the recipient who wishes to hire you as his/her provider (or his/her. Submit your appeal request form. The following are riverside county’s “commonly used ihss forms”. Web sign or have your authorized representative sign, indicate who signed and date your appeal request form. Web the main purpose of this form is to allow an authorized representative to act on behalf of an ihss recipient in matters related to their ihss benefits. A. Web the ihss worker has the responsibility for authorizing services and service hours. Web this document may only be signed by the recipient or by an authorized representative. Web • you (or your authorized representative) must complete part a of this form to let the county know who you have chosen to provide your authorized services. The following are riverside. The following are riverside county’s “commonly used ihss forms”. Submit your appeal request form. Web sign or have your authorized representative sign, indicate who signed and date your appeal request form. Web complete an authorized representative form found at: Web authorized representative means an individual designated by the eligible person receiving services, or by the parent or guardian receiving services,. Web authorized representative means an individual designated by the eligible person receiving services, or by the parent or guardian receiving services, if appropriate, who has the. Web this document may only be signed by the recipient or by an authorized representative. Web sign or have your authorized representative sign, indicate who signed and date your appeal request form. Web the main purpose of this form is to allow an authorized representative to act on behalf of an ihss recipient in matters related to their ihss benefits. Submit your appeal request form. Web the recipient who wishes to hire you as his/her provider (or his/her authorized representative) must submit an ihss recipient request for provider waiver (soc. The information provided in this form will be considered as one factor of the need for. A provider is one who is providing services to an ihss recipient in their home. Web the ihss worker has the responsibility for authorizing services and service hours. The form consists of several. Web • complete a provider enrollment form and bring in original identity documentation and original social security card • complete and pass a doj criminal background check •. Web sign or have your authorized representative sign, indicate who signed and date your appeal request form. You may submitthis form by mail or in person to your ihss county, public authority, or. The following are riverside county’s “commonly used ihss forms”. Submit your appeal request form. Web complete an authorized representative form found at: Web • you (or your authorized representative) must complete part a of this form to let the county know who you have chosen to provide your authorized services.
Authorized Representative Form Sample Fill and Sign Printable

Form Soc 2274 InHome Supportive Services (Ihss ) Program

Alameda Alliance for Health Authorized Representative Form and
Sample Designation Of Authorized Representative Form printable pdf download
Ihss Application Form Pdf Fill Out and Sign Printable PDF Template
Form SOC839 Download Fillable PDF or Fill Online Inhome Supportive
Form SOC 839. InHome Supportive Services (IHSS) Designation Of
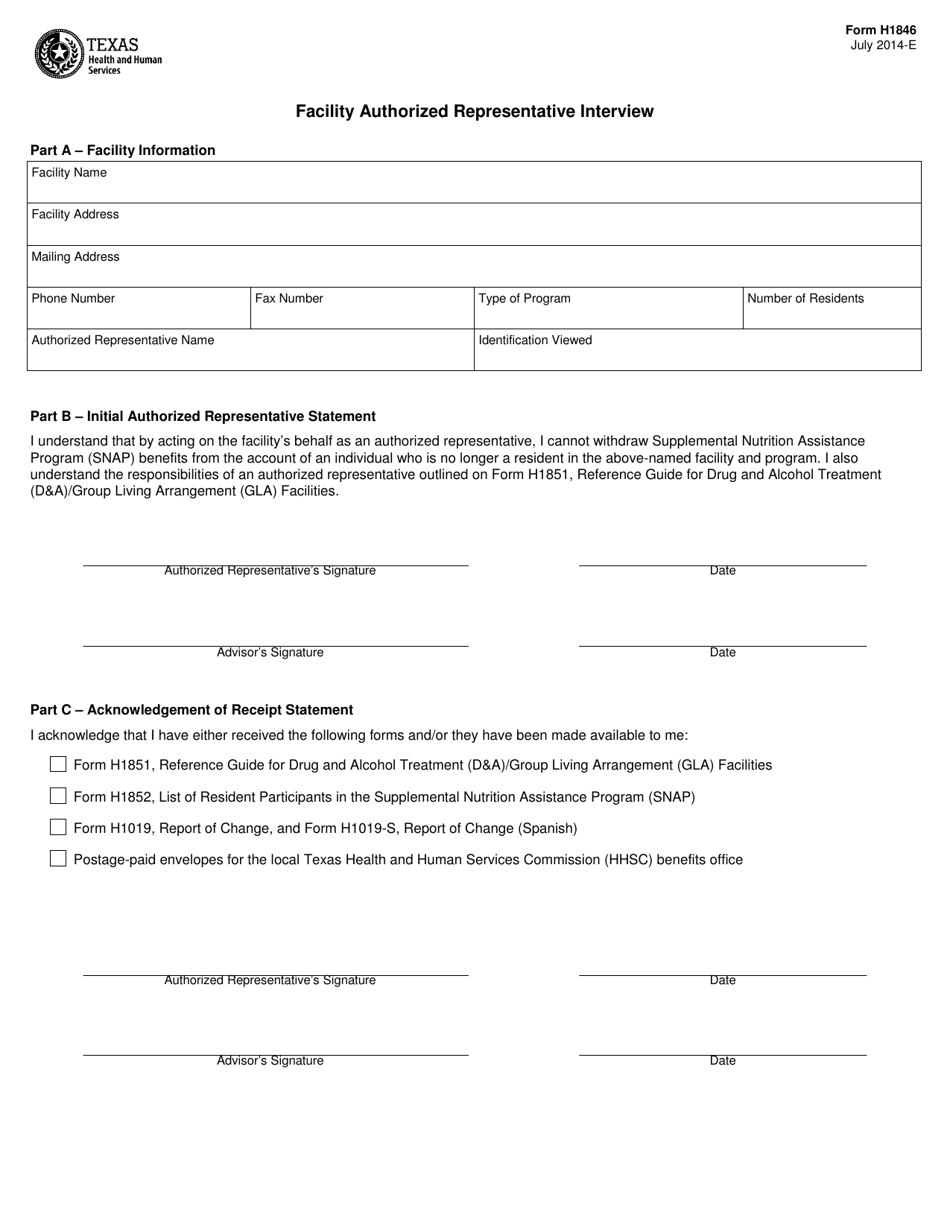
Form H1846 Download Printable PDF or Fill Online Facility Authorized
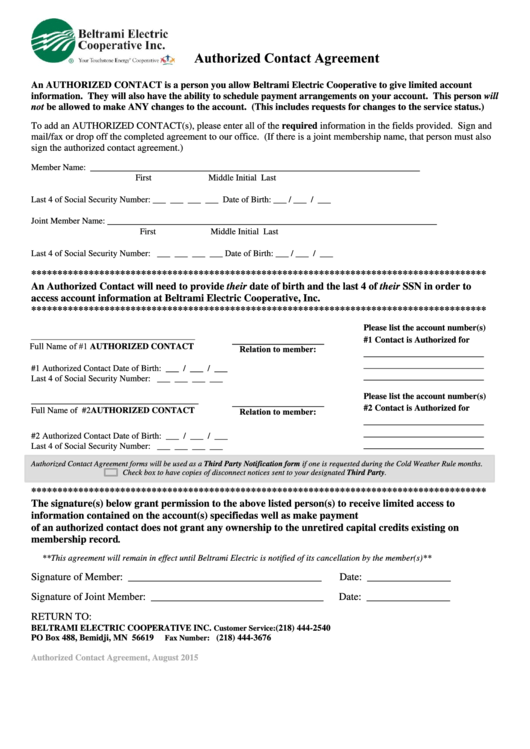
Top 15 Authorized Representative Form Templates free to download in PDF
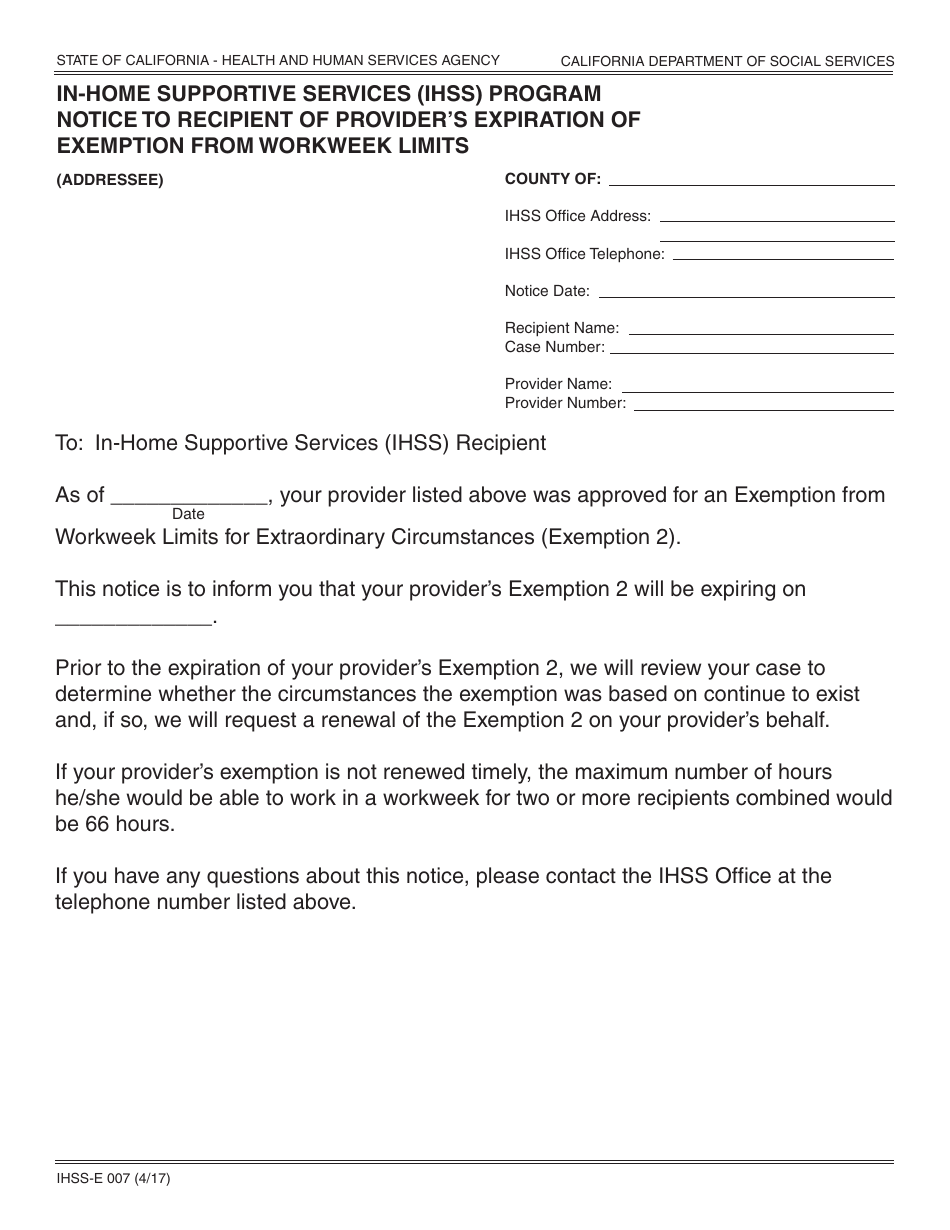
Form IHSSE007 Download Fillable PDF or Fill Online Inhome Supportive
Related Post: