Where To Mail Cms 1763 Form
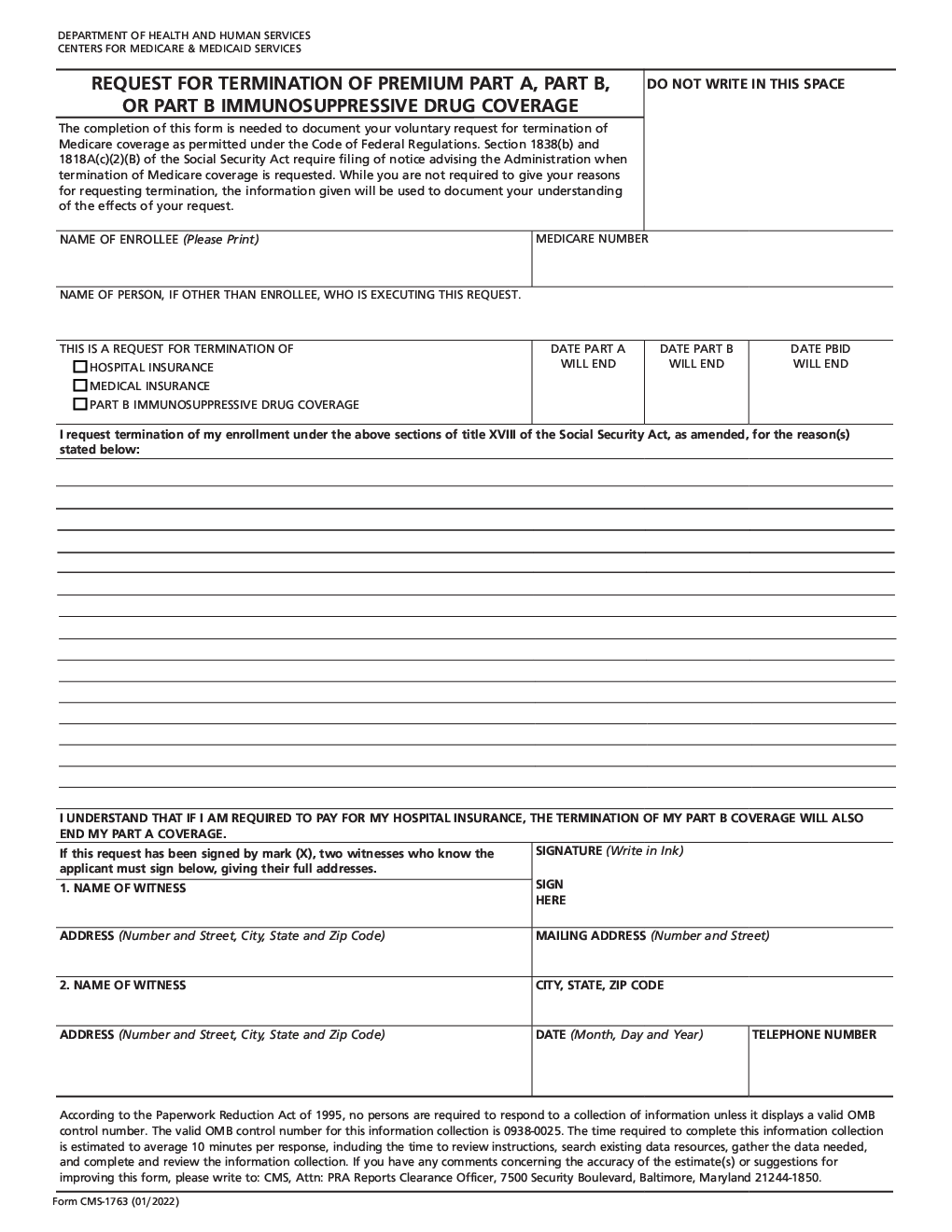
Where To Mail Cms 1763 Form - Or return forms by mail to your local social security office. The fax number and mailing address for your social security form cms 1763 will depend on your location and specific circumstances. Web form # cms 1763. The completion of this form is needed to document your voluntary request for termination of. 05/21) request for termination of premium hospital and/or supplementary medical insurance. Web you can voluntarily terminate your medicare part b (medical insurance). State authorization of qhp data change request form. Web if you'd like to give me your zip code i can get the mailing address for you. Where do i send my medicare form cms 1763? Answered in 5 minutes by: Web hi 00820.901 exhibit 1: Web the cms 1763 form is a legal issued by the centers of medicare and medicaid services that allows medicare recipients to terminate their coverage of premium hospital insurance (premium part a) and/or supplemental medical insurance (part b). The fax number and mailing address for your social security form cms 1763 will depend on your. Request for termination of premium part a, part b, do not write in this space or part b. Web the cms 1763 form is a legal issued by the centers of medicare and medicaid services that allows medicare recipients to terminate their coverage of premium hospital insurance (premium part a) and/or supplemental medical insurance (part b). The fax number and. Learn more vendordatabase 09232013 1217pm. Web form # cms 1763. State authorization of qhp data change request form. You can find this information in the instructions provided with the form or. The centers for medicare & medicaid services (cms) requires, when possible, a. Web form approved omb no. 1568, wb mason, jenny, seltzer, po box 981101. Web hi 00820.901 exhibit 1: Or return forms by mail to your local social security office. 05/21) request for termination of premium hospital and/or supplementary medical insurance. Web hi 00820.901 exhibit 1: I live in redmond wa. Web although form cms 1763 is not available for online submission, you can find it in dochubs library, fill out and easily print it out from your account. Web form # cms 1763. Request for termination of premium hospital insurance of. The centers for medicare & medicaid services (cms) requires, when possible, a. Office of management and budget control number searchable database. Web form # cms 1763. Answered in 5 minutes by: 1568, wb mason, jenny, seltzer, po box 981101. Or return forms by mail to your local social security office. Web i have filled out a cms form 1763 and now i need to know where i cam mail it. Request for termination of premium hospital insurance of supplementary medical insurance: Where do i send my medicare form cms 1763? You may mail written comments to the following address: Web how to fill out cms form 1763 pdffiller 9.77k subscribers subscribe 4k views 1 year ago pdffiller form instructions watch this video to find out how to terminate premium hospital and/or. 05/21) request for termination of premium hospital and/or supplementary medical insurance. However, you may need to have a personal interview with us to review the risks of dropping. 1568, wb mason, jenny, seltzer, po box 981101. 05/21) request for termination of premium hospital and/or supplementary medical insurance. Web form approved omb no. Answered in 5 minutes by: Verified ask your own social security question related social security. However, you may need to have a personal interview with us to review the risks of dropping coverage and for assistance with your request. Verified ask your own social security question related social security. Request for termination of premium part a, part b, do not write in this space or part b. 05/21) request for termination of premium hospital and/or. The completion of this form is needed to document your voluntary request for termination of. Request for termination of premium part a, part b, do not write in this space or part b. Office of management and budget control number searchable database. Web how to fill out cms form 1763 pdffiller 9.77k subscribers subscribe 4k views 1 year ago pdffiller form instructions watch this video to find out how to terminate premium hospital and/or. Web i have filled out a cms form 1763 and now i need to know where i cam mail it. Web the cms 1763 form is a legal issued by the centers of medicare and medicaid services that allows medicare recipients to terminate their coverage of premium hospital insurance (premium part a) and/or supplemental medical insurance (part b). Or return forms by mail to your local social security office. You can find this information in the instructions provided with the form or. 1568, wb mason, jenny, seltzer, po box 981101. However, you may need to have a personal interview with us to review the risks of dropping coverage and for assistance with your request. • cms form filing requires the. State authorization of qhp data change request form. Web form # cms 1763. The centers for medicare & medicaid services (cms) requires, when possible, a. Web you can voluntarily terminate your medicare part b (medical insurance). Request for termination of premium hospital insurance of. Web form approved omb no. Where do i send my medicare form cms 1763? Request for termination of premium hospital insurance of supplementary medical insurance: Can i also email the form instead of mailing it?
Printable Form Cms 1763 Printable World Holiday

Cms 1763 Printable Form Printable Forms Free Online
Cms 1763 Form 2006 Fill Out and Sign Printable PDF Template signNow
Medicare Form 1490S Fill Out and Sign Printable PDF Template signNow
CMS 1763 Form Medicare Form CMS 1763 blank, sign online — PDFliner
CMS 1763
Where Do I Mail Medicare Form Cms 1763 Form Resume Examples AjYdXvKoYl
Printable Form Cms 1763 Printable World Holiday

Medicare, Social Security, and Form CMS 1763 PDFfiller Blog
CMS 1763. Request for Termination of Premium Hospital Insurance of
Related Post: