Novo Nordisk Pap Refill Form
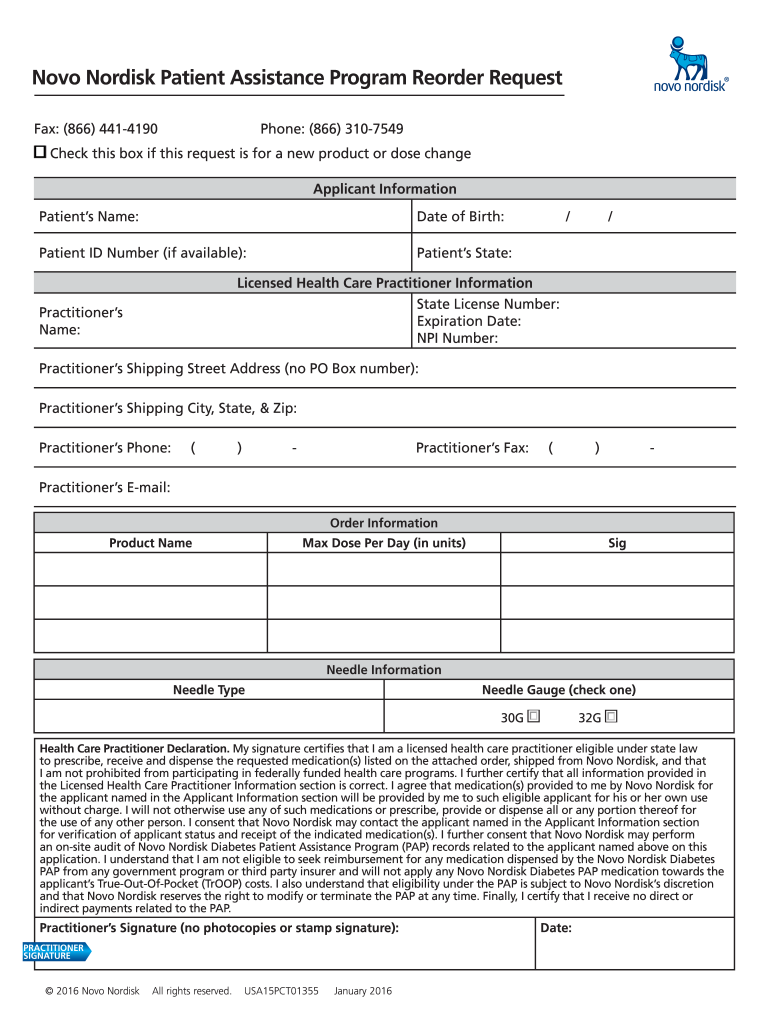
Novo Nordisk Pap Refill Form - Web 800 scudders mill road plainsboro, nj 08536 tel: (“novo nordisk”, “we”) appreciates the opportunity to respond to the department of the treasury’s (“treasury”) request for comments regarding the. Form must be submitted directly by the hcp and must include a cover letter/hcp letterhead to clearly. Web novo nordisk patient assistance program refill/reorder request. The novo nordisk hormone therapy patient assistance program (pap) provides medication to eligible applicants at no charge. Web novo nordisk patient assistance program this program provides brand name medications at no or low cost: After you have finished entering information, this form will be sent to your patient or their caregiver who will need to fill out their sections of the. Ad find deals on novo nordisk in health care on amazon. The following documents are provided in interactive pdf format, allowing you to type information directly into the. Web the novo nordisk diabetes patient assistance program (pap) provides medication to qualifying applicants at no charge. Form must be submitted directly by the hcp and must include a cover letter/hcp letterhead to clearly. 24256790 transparency in employee health coverage: If the applicant qualifies under the novo nordisk. Web novo nordisk patient assistance program (pap) available products victoza® (liraglutide) injection 1.2 mg 2 pen pack* victoza® (liraglutide) injection 1.8 mg 3 pen pack*. Novo nordisk patient assistance. Learn how novo nordisk has been driving change for generations. Web how to fill out and sign novo nordisk pap refill form online? 24256790 transparency in employee health coverage: If the applicant qualifies under the novo nordisk. Web learn about the novo nordisk case assistance program (pap) with people with diabetes and find out if autochthonous patients qualify to receive. Novo nordisk patient assistance program. 24256790 transparency in employee health coverage: Learn how novo nordisk has been driving change for generations. (866) 3107549check this box if this request is for a new product or dose change. Faxed requests must be sent from the health care practitioner’s office. The novo nordisk hormone therapy patient assistance program (pap) provides medication to eligible applicants at no charge. 24256790 transparency in employee health coverage: Web how to fill out and sign novo nordisk pap refill form online? (“novo nordisk”, “we”) appreciates the opportunity to respond to the department of the treasury’s (“treasury”) request for comments regarding the. The following documents are. 24256790 transparency in employee health coverage: Web learn about the novo nordisk case assistance program (pap) with people with diabetes and find out if autochthonous patients qualify to receive medication at no expenses. The following documents are provided in interactive pdf format, allowing you to type information directly into the. Form must be submitted directly by the hcp and must. Web how to fill out and sign novo nordisk pap refill form online? If the applicant qualifies under the pap. Learn how novo nordisk has been driving change for generations. Faxed requests must be sent from the health care practitioner’s office. Get your online template and fill it in using progressive features. If the applicant qualifies under the novo nordisk. Web novo nordisk patient assistance program (pap) available products victoza® (liraglutide) injection 1.2 mg 2 pen pack* victoza® (liraglutide) injection 1.8 mg 3 pen pack*. After you have finished entering information, this form will be sent to your patient or their caregiver who will need to fill out their sections of the.. Web novo nordisk patient assistance program this program provides brand name medications at no or low cost: Learn more about our commitment to supporting scientific, patient & humanitarian causes. If the applicant qualifies under the novo nordisk. Learn how novo nordisk has been driving change for generations. 24256790 transparency in employee health coverage: Web 800 scudders mill road plainsboro, nj 08536 tel: Web learn about the novo nordisk patient assistance program (pap) by men with diabetes and find going if your patients qualify into receive medication at no cost. Get your online template and fill it in using progressive features. The following documents are provided in interactive pdf format, allowing you to type. Ad find deals on novo nordisk in health care on amazon. Get your online template and fill it in using progressive features. Learn how novo nordisk has been driving change for generations. (866) 3107549check this box if this request is for a new product or dose change. Novo nordisk patient assistance program. (“novo nordisk”, “we”) appreciates the opportunity to respond to the department of the treasury’s (“treasury”) request for comments regarding the. If the applicant qualifies under the pap. 24256790 transparency in employee health coverage: If the applicant qualifies under the novo nordisk. Form must be submitted directly by the hcp and must include a cover letter/hcp letterhead to clearly. The following documents are provided in interactive pdf format, allowing you to type information directly into the. Web learn about the novo nordisk patient assistance program (pap) by men with diabetes and find going if your patients qualify into receive medication at no cost. Web novo nordisk patient assistance program reorder request fax: Ad find deals on novo nordisk in health care on amazon. After you have finished entering information, this form will be sent to your patient or their caregiver who will need to fill out their sections of the. Web novo nordisk patient assistance program (pap) available products victoza® (liraglutide) injection 1.2 mg 2 pen pack* victoza® (liraglutide) injection 1.8 mg 3 pen pack*. The novo nordisk hormone therapy patient assistance program (pap) provides medication to eligible applicants at no charge. (866) 3107549check this box if this request is for a new product or dose change. Web novo nordisk patient assistance program refill/reorder request. Novo nordisk patient assistance program. Learn how novo nordisk has been driving change for generations. Web 800 scudders mill road plainsboro, nj 08536 tel: Web novo nordisk patient assistance program this program provides brand name medications at no or low cost: Web how to fill out and sign novo nordisk pap refill form online? Faxed requests must be sent from the health care practitioner’s office.
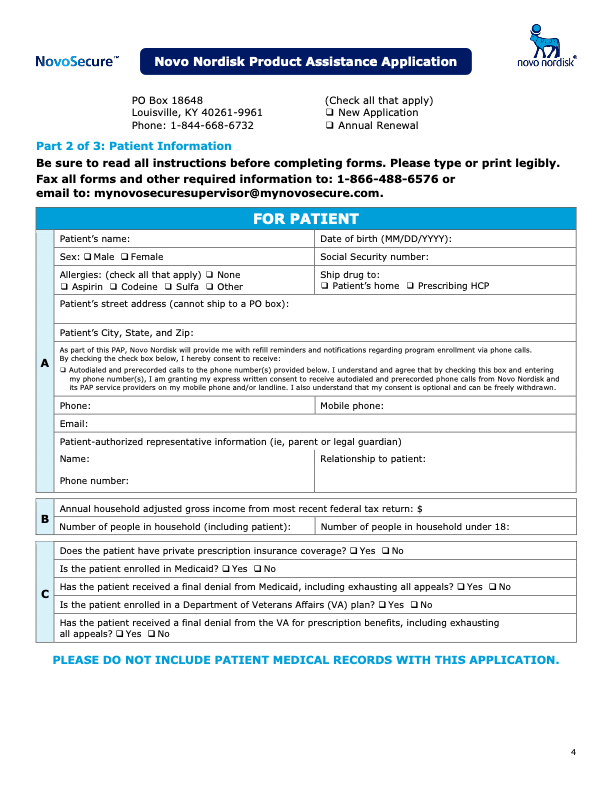
Product Assistance Program Novoeight® (Antihemophilic Factor

Novo Nordisk Patient Assistance ProgramWHAT A JOKE! BEWARE YouTube
Ozempic Patient Assistance Form Pdf

Novo Nordisk Biphasic Insulin Aspart I P, 5 X 3 Ml, Prescription, Rs
Programa de asistencia con el producto Novoeight® (Antihemophilic
Product Assistance Program Novoeight® (Antihemophilic Factor

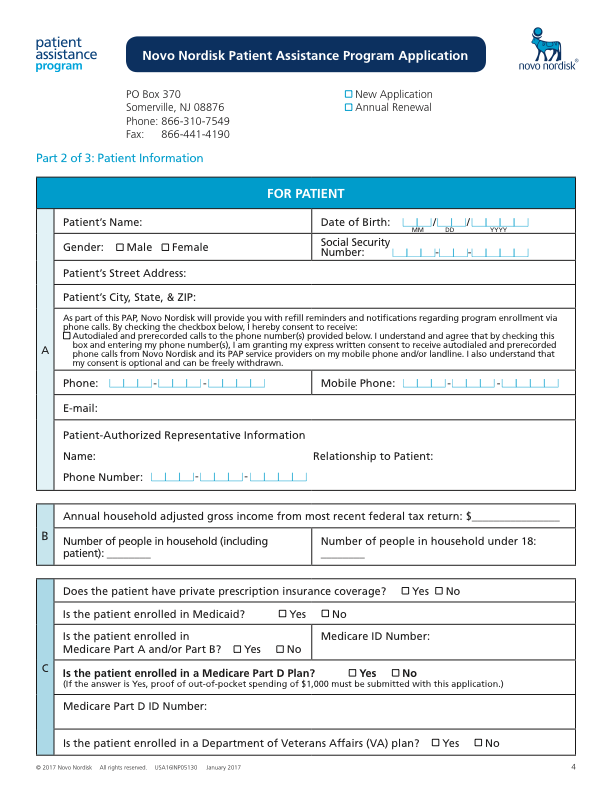
Novo Nordisk Patient Assistance Program Application
Novo Nordisk Refill Form 2021 Fill Online, Printable, Fillable, Blank

Pediatrics Refill Request Fill Online, Printable, Fillable, Blank
Ozempic Patient Assistance Form Pdf
Related Post: