Medicare Part D Coverage Determination Request Form
Medicare Part D Coverage Determination Request Form - Web get the right medicare drug plan for you. Overview of what medicare drug plans cover. Web cms has posted a model form (“request for medicare prescription drug coverage determination”) to assist part d enrollees in asking their medicare drug plans for a. Web a coverage determination is any decision made by the part d plan sponsor regarding: Web request for medicare prescription drug coverage determination this form may be sent to us by mail or fax: Ad thinking about switching medicare plans? What medicare part d drug plans cover. Pay no more than $35/month's supply for each covered insulin. Web coverage determination request. 711), 24 hours a day, 7 days a week, or through our website at. Web medicare part d coverage determination request form (pdf) (387.51 kb) (for use by members and doctors/providers) for certain requests, you'll also need a supporting. Web coverage determination request. Make sure your 2024 plan covers your insulin and all your rx needs. If your income is greater than $103,000 and less than $397,000, the irmaa amount is $74.20. Everyone who. Web section 1871(a)(2) of the act provides that no rule, requirement, or other statement of policy (other than a national coverage determination) that establishes or. Web get the right medicare drug plan for you. Web a coverage determination is any decision made by the part d plan sponsor regarding: Web medicare part d coverage determination request form (pdf) (387.51 kb). Web enrollee’s part d plan id number requestor’s name (if not enrollee) requestor’s relationship to enrollee (attach documentation that shows authority to represent enrollee,. Pay no more than $35/month's supply for each covered insulin. Web medicare is split into parts a, b, c and d. Web medicare part d coverage determination request form is a form used by medicare beneficiaries. Pay no more than $35/month's supply for each covered insulin. Receipt of, or payment for, a prescription drug that an enrollee believes may. Make sure your 2024 plan covers your insulin and all your rx needs. Web medicare part d coverage determination request form (pdf) (387.51 kb) (for use by members and doctors/providers) for certain requests, you'll also need a. Overview of what medicare drug plans cover. Ad thinking about switching medicare plans? Everyone who works contributes, through their payroll taxes, to the funds that pay for medicare. Web use this form to request a coverage determination, including an exception, from a plan sponsor, for your medicare part d coverage. Web cms has posted a model form (“request for medicare. Web part b coverage. Web section 1871(a)(2) of the act provides that no rule, requirement, or other statement of policy (other than a national coverage determination) that establishes or. Web get medicare forms for different situations, like filing a claim or appealing a coverage decision. Web request for medicare prescription drug coverage determination this form may be sent to us. If your income is greater than $103,000 and less than $397,000, the irmaa amount is $74.20. Web enrollee’s part d plan id number requestor’s name (if not enrollee) requestor’s relationship to enrollee (attach documentation that shows authority to represent enrollee,. Web medicare part d coverage determination request form (pdf) (387.51 kb) (for use by members and doctors/providers) for certain requests,. Web you cannot request an expedited coverage determination if you are asking us to pay you back for a drug you already received. Web request for medicare prescription drug coverage determination this form may be sent to us by mail or fax: Web cms has posted a model form (“request for medicare prescription drug coverage determination”) to assist part d. Learn about formularies, tiers of. Web a coverage determination is an initial coverage decision made by scan regarding your medicare part d prescription drug. Receipt of, or payment for, a prescription drug that an enrollee believes may. Ad need a medicare plan that meets your health needs? What medicare part d drug plans cover. Web get the right medicare drug plan for you. Wisdom comes with benefits, like knowing to choose a part d plan with cigna healthcare. A request to change the amount you must pay for a health care service, supply, item, or. Receipt of, or payment for, a prescription drug that an enrollee believes may. Ad need a medicare plan that. Web enrollee’s part d plan id number requestor’s name (if not enrollee) requestor’s relationship to enrollee (attach documentation that shows authority to represent enrollee,. Receipt of, or payment for, a prescription drug that an enrollee believes may. Web section 1871(a)(2) of the act provides that no rule, requirement, or other statement of policy (other than a national coverage determination) that establishes or. Web you cannot request an expedited coverage determination if you are asking us to pay you back for a drug you already received. Providers may request a coverage decision and/or exception any of the following ways: A request to change the amount you must pay for a health care service, supply, item, or. Ad need a medicare plan that meets your health needs? Web part b coverage. Web request for medicare prescription drug coverage determination this form may be sent to us by mail or fax: Licensed insurance agents are ready to help you compare your medicare plan options. You can also ask for a faster (expedited) initial. Make sure your 2024 plan covers your insulin and all your rx needs. Web included in the downloads section below are links to forms applicable to part d grievances, coverage determinations (including exceptions) and appeals. Web 2 days agooctober 15: Web coverage determination request. Web a coverage determination is any decision made by the part d plan sponsor regarding: Receipt of, or payment for, a prescription drug that an enrollee believes may. Ad cigna healthcare offers prescription drug plans to fit your health needs. Web a coverage determination is any decision made by the part d plan sponsor regarding: Web medicare part d coverage determination request form.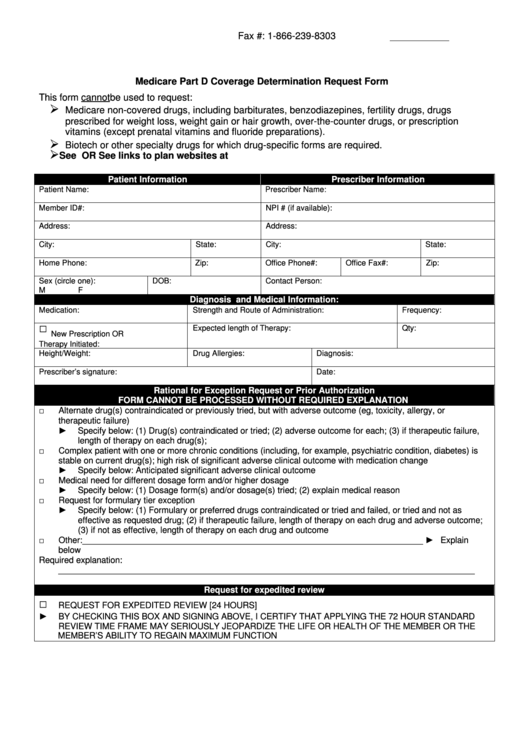
Medicare Part D Coverage Determination Request Form printable pdf download
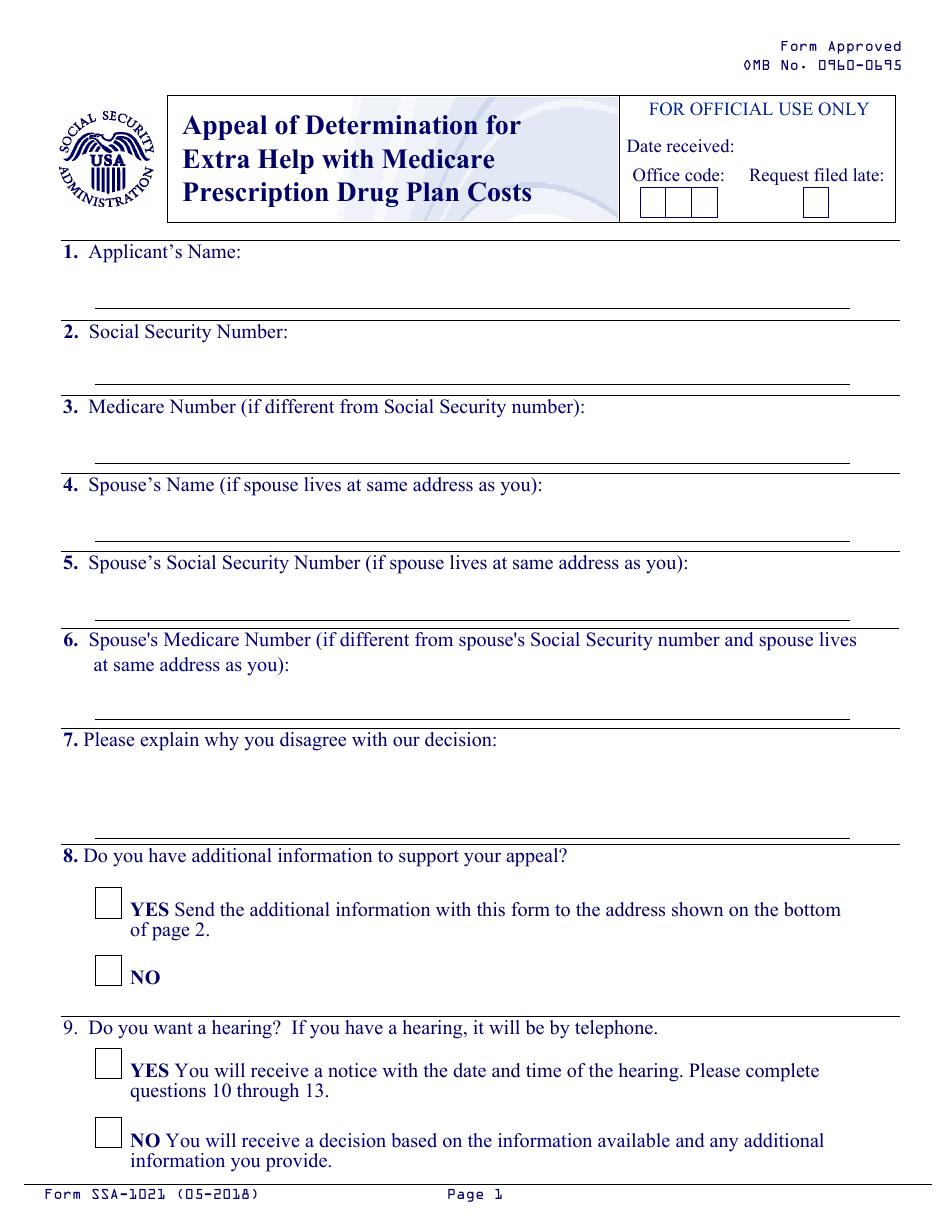
Form SSA1021 Fill Out, Sign Online and Download Fillable PDF
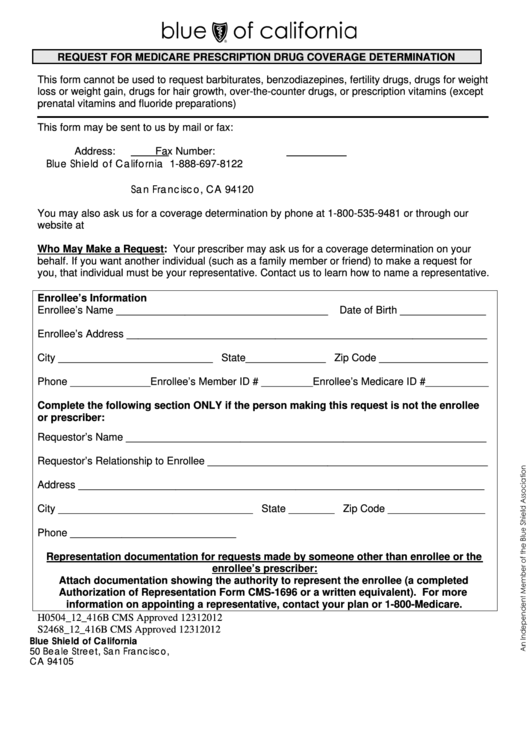
Request For Medicare Prescription Drug Coverage Determination Form

Wellcare medicare request for prescription drug coverage determination
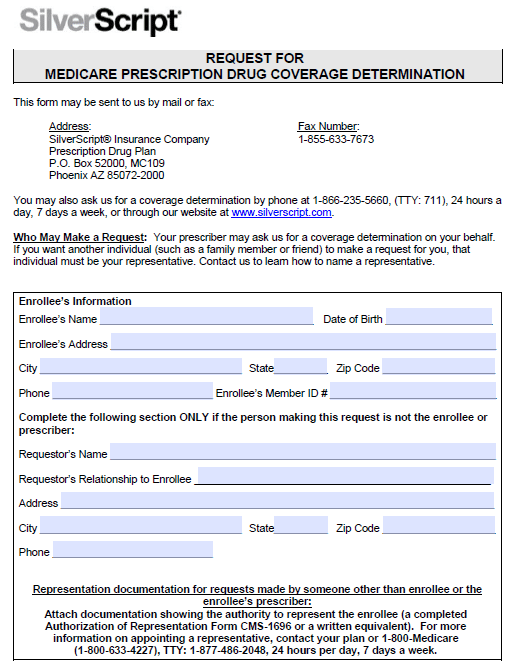
Free SilverScript Prior Prescription (Rx) Authorization Form PDF

Wellcare Medicare Part D Coverage Determination Request Form Form

Wellcare Medicare Part D Coverage Determination Request Form Form
Wellcare Medicare Part D Tier Exception Form Form Resume Examples
Medicare Part D Coverage Determination Request Form Form Resume
Aetna Appeal Form 2023 Fill Out and Sign Printable PDF Template signNow
Related Post: