Ihss Provider Form
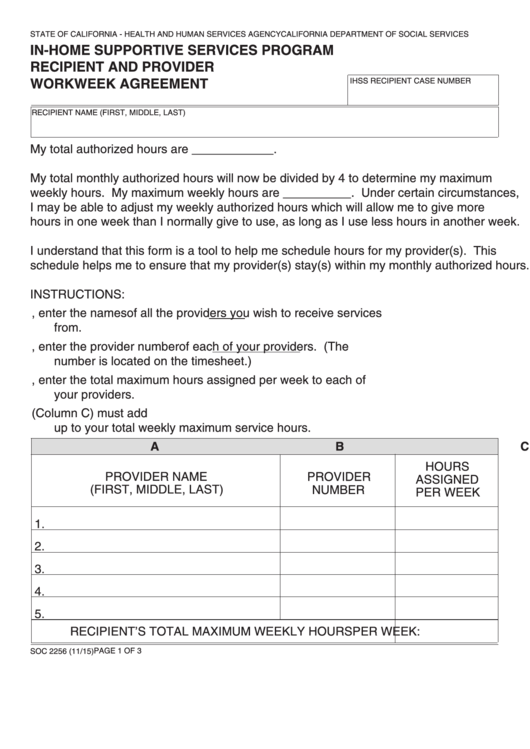
Ihss Provider Form - Give the original copy to your client; Provider name (first, middle, last). Ihss providers can be paid to accompany. Notifying the county ihss office within 10 days when i hire or fire a provider. Web fresno ihss care providers can choose from the available forms to provide information, keep their information current, or request changes. Web to provide information for your application: Beginning july 1, 2023, you will. You can earn paid sick leave if you're an active provider working for an ihss/wpcs recipient. 3) referring any individual i want to hire to the county ihss office to complete the provider eligibility process. Submit issues to ihss staff, upload documents, and check status of existing issues. You can earn paid sick leave if you're an active provider working for an ihss/wpcs recipient. Submit issues to ihss staff, upload documents, and check status of existing issues. Web fresno ihss care providers can choose from the available forms to provide information, keep their information current, or request changes. Complete the ihss provider enrollment forms. In addition, i understand. Web my ihss authorized hours each month. Paid sick leave for providers. Web you must have a physician or other licensed health care professional fill out a health care certification form and you must return it to the county before care services can be. Provider number provider enrollment agreement. You have the right to interpreter services provided by the county. Web to provide information for your application: 3) referring any individual i want to hire to the county ihss office to complete the provider eligibility process. California department of social services. Ad iluvenglish.com has been visited by 10k+ users in the past month In addition, i understand and agree to the following terms and limitations regarding payment for. Provider number provider enrollment agreement. Web fresno ihss care providers can choose from the available forms to provide information, keep their information current, or request changes. You have the right to interpreter services provided by the county at no. Ihss providers can be paid to accompany. You can earn paid sick leave if you're an active provider working for an. English armenian cambodian chinese farsi korean russian spanish. You can earn paid sick leave if you're an active provider working for an ihss/wpcs recipient. Provider number provider enrollment agreement. Web fresno ihss care providers can choose from the available forms to provide information, keep their information current, or request changes. Provider name (first, middle, last). Provider number provider enrollment agreement. You can earn paid sick leave if you're an active provider working for an ihss/wpcs recipient. Ihss providers can be paid to accompany. Web you must have a physician or other licensed health care professional fill out a health care certification form and you must return it to the county before care services can be.. Notifying the county ihss office within 10 days when i hire or fire a provider. In addition, i understand and agree to the following terms and limitations regarding payment for. Web fresno ihss care providers can choose from the available forms to provide information, keep their information current, or request changes. Provider number provider enrollment agreement. Web to provide information. Complete the ihss provider enrollment forms. Provider name (first, middle, last). Give the original copy to your client; In addition, i understand and agree to the following terms and limitations regarding payment for. English armenian cambodian chinese farsi korean russian spanish. California department of social services. Paid sick leave for providers. Web you must have a physician or other licensed health care professional fill out a health care certification form and you must return it to the county before care services can be. English armenian cambodian chinese farsi korean russian spanish. Web fresno ihss care providers can choose from the available. Paid sick leave for providers. Provider name (first, middle, last). California department of social services. Ad iluvenglish.com has been visited by 10k+ users in the past month Web to provide information for your application: Notifying the county ihss office within 10 days when i hire or fire a provider. California department of social services. Web you must have a physician or other licensed health care professional fill out a health care certification form and you must return it to the county before care services can be. Web to provide information for your application: 3) referring any individual i want to hire to the county ihss office to complete the provider eligibility process. Provider number provider enrollment agreement. In addition, i understand and agree to the following terms and limitations regarding payment for. Complete the ihss provider enrollment forms. Give the original copy to your client; Provider name (first, middle, last). Ihss providers can be paid to accompany. Ad iluvenglish.com has been visited by 10k+ users in the past month Submit issues to ihss staff, upload documents, and check status of existing issues. You have the right to interpreter services provided by the county at no. Web fresno ihss care providers can choose from the available forms to provide information, keep their information current, or request changes. You can earn paid sick leave if you're an active provider working for an ihss/wpcs recipient. English armenian cambodian chinese farsi korean russian spanish. Web my ihss authorized hours each month. Paid sick leave for providers. Your client must sign and date.
In home supportive services application form
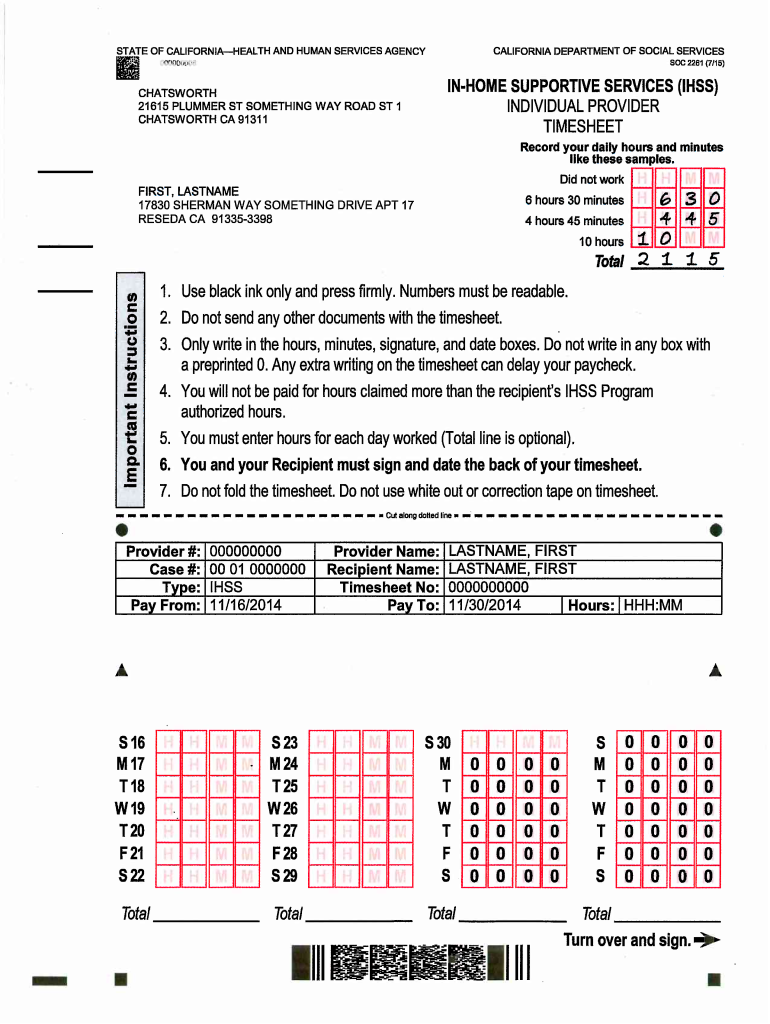
California IHSS Individual Provider Timesheet Form (SOC 2261) DocHub
How to a ihss provider in ga form Fill out & sign online DocHub

Form Soc 2274 InHome Supportive Services (Ihss ) Program

Ihss Provider Application Form Form Resume Examples gq9608lVOR

Ihss Provider Timesheet Status Timesheet template, Statement template
Top 17 Ihss Forms And Templates free to download in PDF format
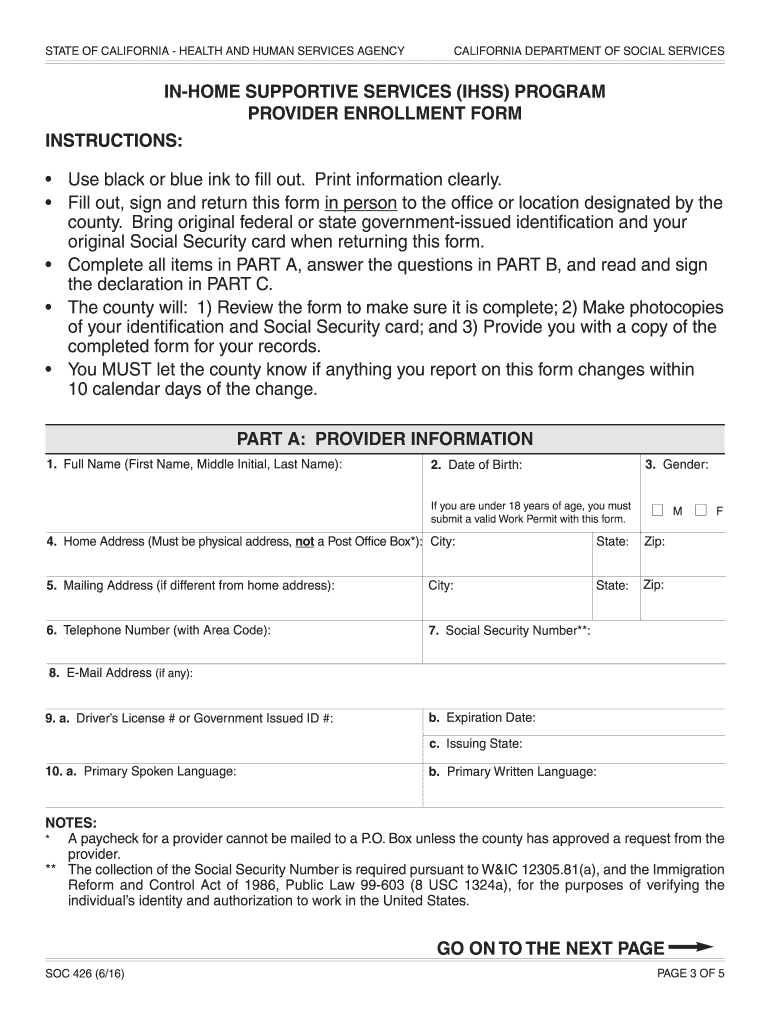
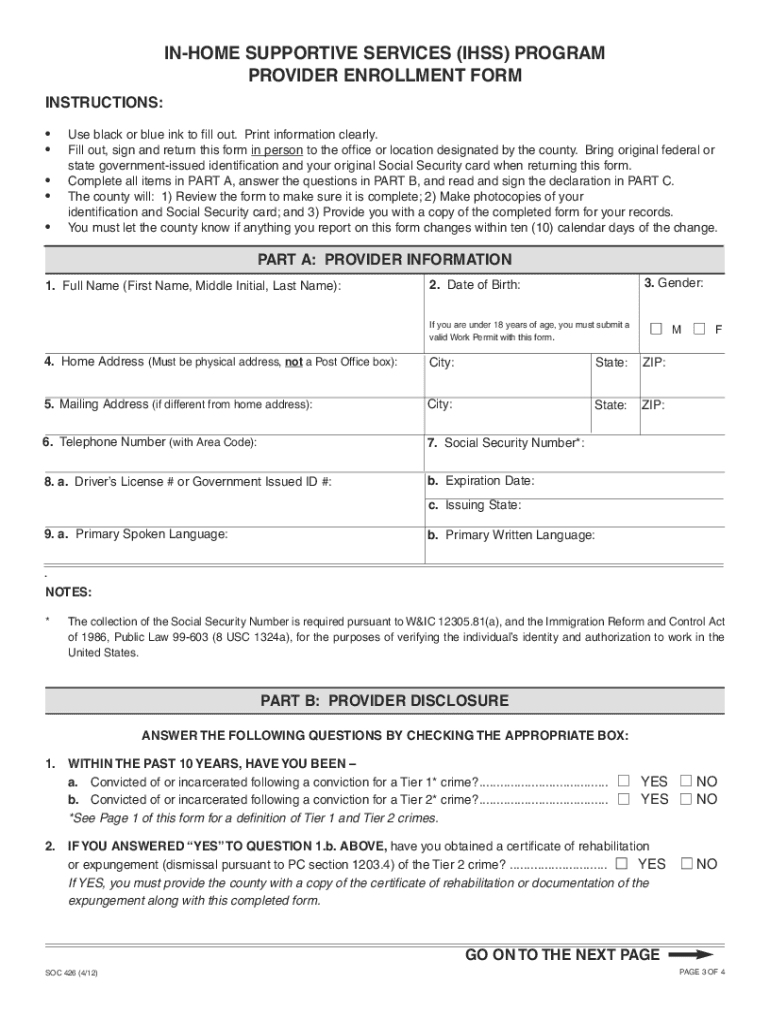
Ihss program provider enrollment form soc 426 Fill out & sign online
Fillable Form Soc 2271 InHome Supportive Services (Ihss) Program

Ihss Provider Enrollment Form Soc 426 Form Resume Examples Wk9yjW0Y3D
Related Post: