Ihss Change Provider Form
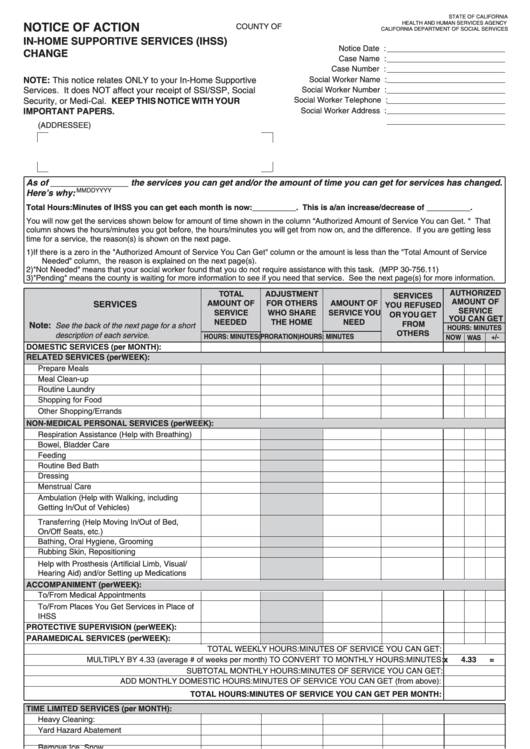
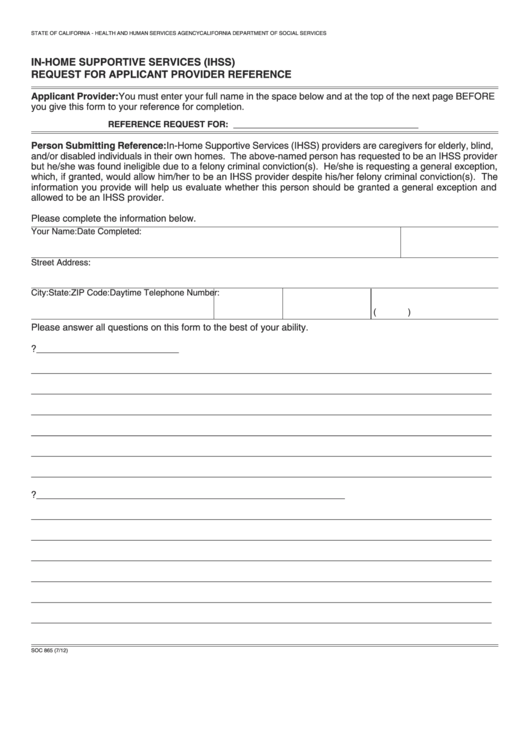
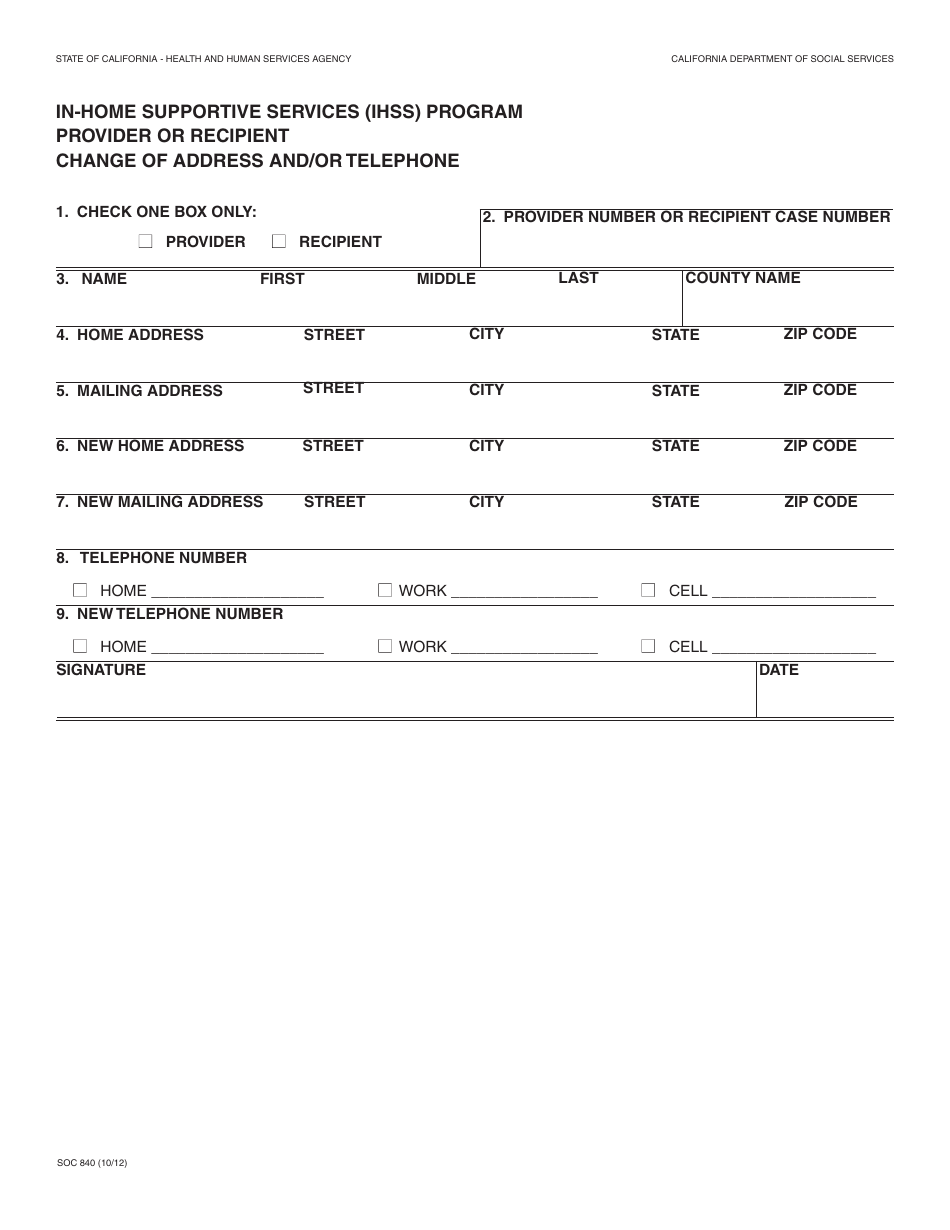
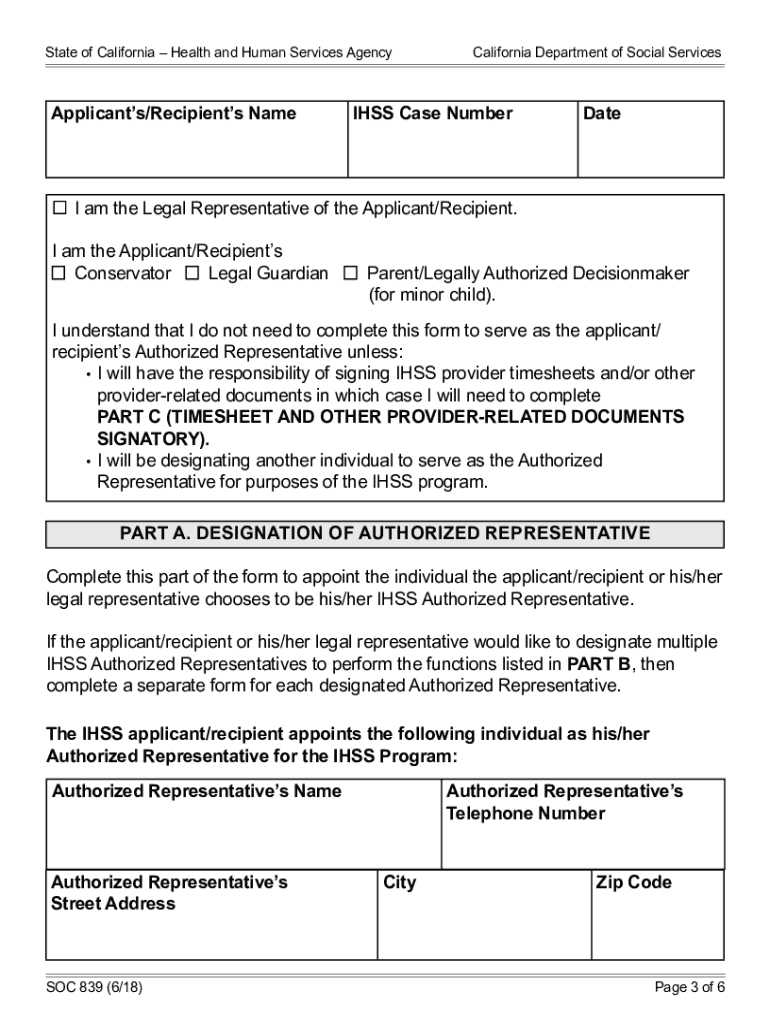
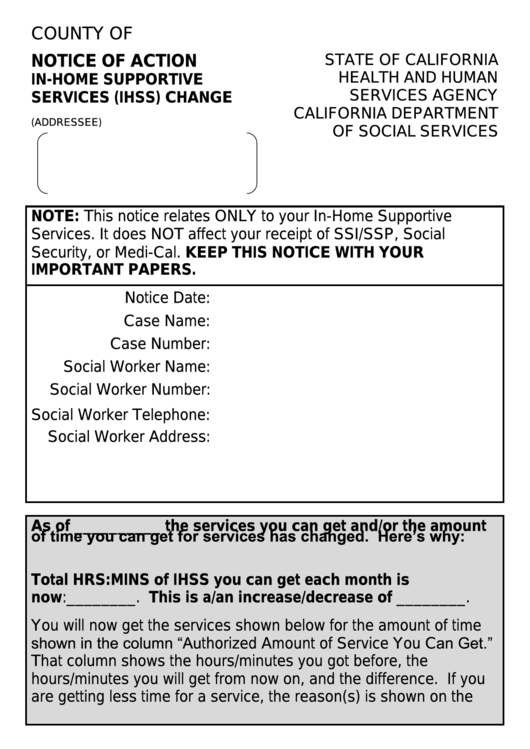
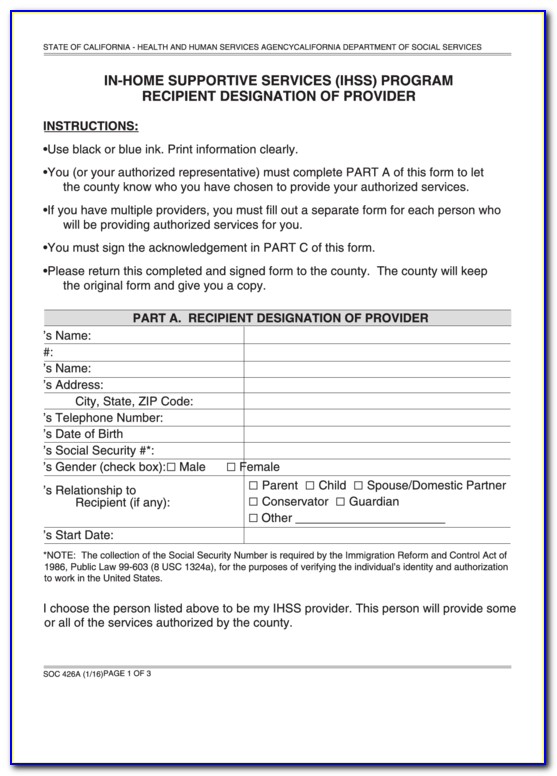
Ihss Change Provider Form - Services are provided in your home, hotel, or the home of a. The consumer can obtain this form by contacting your. Web the online direct deposit enrollment service allows current, active ihss/wpcs providers in all california counties the ability to electronically enroll,. Notifying the county ihss office within 10 days when i hire or fire a provider. Beginning july 1, 2023, you will. The first step in the process is to complete and sign the ihss program provider enrollment. The appropriate cdss form to. Web you must submit a completed health care certification form. In addition, i understand and agree to the following terms and limitations regarding payment for. It typically includes information such as your name, contact details,. In addition, i understand and agree to the following terms and limitations regarding payment for. The appropriate cdss form to. Web wish to change or cancel your direct deposit authorization for any recipient for whom you work, you must submit an enrollment/change/cancellation form with a check next to. A new address and/or phone number are required to be reported within. Web you must submit a completed health care certification form. Web below details how to change your address with ihss. The appropriate cdss form to. Web ihss provider change form: The consumer can obtain this form by contacting your. English armenian cambodian chinese farsi korean russian spanish. A new address and/or phone number are required to be reported within 10 days of the change. The first step in the process is to complete and sign the ihss program provider enrollment. Beginning july 1, 2023, you will. Notifying the county ihss office within 10 days when i hire or fire. Beginning july 1, 2023, you will. English armenian cambodian chinese farsi korean russian spanish. Web you must submit a completed health care certification form. It typically includes information such as your name, contact details,. More information on ihss recipients. Notifying the county ihss office within 10 days when i hire or fire a provider. Web the online direct deposit enrollment service allows current, active ihss/wpcs providers in all california counties the ability to electronically enroll,. You have the right to interpreter services provided by the county at no. This is the primary document where you request a change in. The first step in the process is to complete and sign the ihss program provider enrollment. Web you must submit a completed health care certification form. You can earn paid sick leave if you're an active provider working for an ihss/wpcs recipient. This is the primary document where you request a change in your ihss provider. Web ihss provider change. In addition, i understand and agree to the following terms and limitations regarding payment for. The first step in the process is to complete and sign the ihss program provider enrollment. The consumer can obtain this form by contacting your. Change of address in spanish. Change of address in english. Services are provided in your home, hotel, or the home of a. Change of address in spanish. Web you must submit a completed health care certification form. Web fresno ihss care providers can choose from the available forms to provide information, keep their information current, or request changes. You have the right to interpreter services provided by the county at. English armenian cambodian chinese farsi korean russian spanish. Change of address in english. In addition, i understand and agree to the following terms and limitations regarding payment for. It typically includes information such as your name, contact details,. You can earn paid sick leave if you're an active provider working for an ihss/wpcs recipient. The first step in the process is to complete and sign the ihss program provider enrollment. Web fresno ihss care providers can choose from the available forms to provide information, keep their information current, or request changes. You have the right to interpreter services provided by the county at no. A new address and/or phone number are required to be. Web ihss provider change form: Beginning july 1, 2023, you will. The first step in the process is to complete and sign the ihss program provider enrollment. Paid sick leave for providers. The ihss helpline community offers. English armenian cambodian chinese farsi korean russian spanish. This is the primary document where you request a change in your ihss provider. Notifying the county ihss office within 10 days when i hire or fire a provider. You can earn paid sick leave if you're an active provider working for an ihss/wpcs recipient. You have the right to interpreter services provided by the county at no. More information on ihss recipients. Web fresno ihss care providers can choose from the available forms to provide information, keep their information current, or request changes. Web you must submit a completed health care certification form. A new address and/or phone number are required to be reported within 10 days of the change. In addition, i understand and agree to the following terms and limitations regarding payment for. Services are provided in your home, hotel, or the home of a. The appropriate cdss form to. Web the online direct deposit enrollment service allows current, active ihss/wpcs providers in all california counties the ability to electronically enroll,. The consumer can obtain this form by contacting your. Change of address in spanish.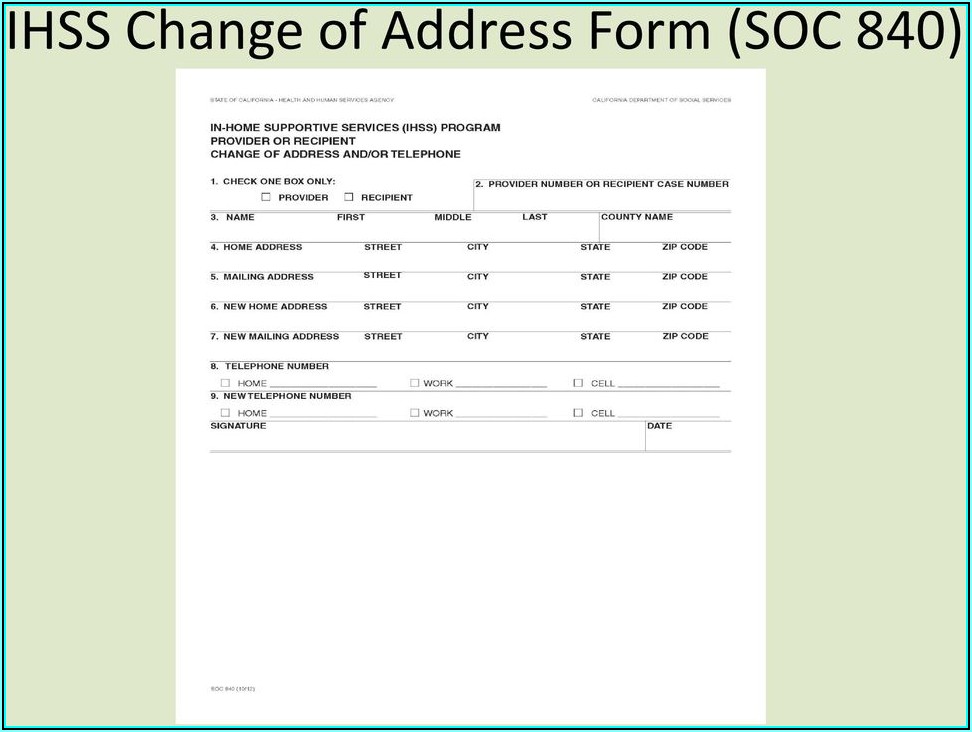
Ihss Provider Enrollment Form Soc 426 Form Resume Examples Wk9yjW0Y3D

Form SOC2312A Download Fillable PDF or Fill Online Inhome Supportive
Fillable Form Na 1253 Notice Of Action InHome Supportive Services
Fillable Form Soc 865 InHome Supportive Services (Ihss) Request For
Ihss New Provider Enrollment Form Los Angeles Enrollment Form
Form SOC840 Fill Out, Sign Online and Download Fillable PDF
Ihss In Home Supportive Services Fill Online, Printable, Fillable
Form Na 1253l Notice Of Action InHome Supportive Services (Ihss
Ihss Provider Address Change Form Form Resume Examples a15qX6aDeQ
Ihss Provider Address Change Form Form Resume Examples a15qX6aDeQ
Related Post: