Ihss Change Of Provider Form
Ihss Change Of Provider Form - Web please review the provider notice and request form below for additional information. Web forms forms implementation of overtime and travel pay require a number of new forms to be completed by both ihss recipients and providers. Obtain the request for live scan service form to get a criminal background check. Web the recipient who wishes to hire you as his/her provider (or his/her authorized representative) must submit an ihss recipient request for provider waiver (soc 862). English armenian cambodian chinese farsi korean russian spanish. This form allows you to. Web the appropriate cdss form to download and fill out is the soc 840 ihss program provider or recipient change of address and/or telephone. Web individuals wanting a claims status; Web soc 840 ihss provider or recipient change of address and/or telephone english armenian cambodian chinese farsi korean russian spanish tagalog vietnamese soc. For press inquiries please contact our public affairs office at. Web individuals wanting a claims status; Web please review the provider notice and request form below for additional information. Web forms forms implementation of overtime and travel pay require a number of new forms to be completed by both ihss recipients and providers. The first step in the process is to complete and sign the ihss program provider enrollment. Web. Web the appropriate cdss form to download and fill out is the soc 840 ihss program provider or recipient change of address and/or telephone. Begin the enrollment process by. Web to add or change a provider, the consumer must call their provider clerk. Web wish to change or cancel your direct deposit authorization for any recipient for whom you work,. Web the ihs is the principal federal health care provider and health advocate for indian people, and provides a comprehensive health service delivery system for american indians and. A friend, a neighbor, or a professional caregiver. The first step in the process is to complete and sign the ihss program provider enrollment. Begin the enrollment process by. For press inquiries. The below form (s) are required,. All new ihss providers (i.e., providers who are not currently working for any consumers) must be. The first step in the process is to complete and sign the ihss program provider enrollment. A new address and/or phone number are required to be reported within 10 days of the change. Web forms forms implementation of. A new address and/or phone number are required to be reported within 10 days of the change. Web to add or change a provider, the consumer must call their provider clerk. Web the ihs is the principal federal health care provider and health advocate for indian people, and provides a comprehensive health service delivery system for american indians and. The. Web to add or change a provider, the consumer must call their provider clerk. Web complete and return the required enrollment forms; The below form (s) are required,. The first step in the process is to complete and sign the ihss program provider enrollment. Web please review the provider notice and request form below for additional information. The ihss helpline community offers. Web wish to change or cancel your direct deposit authorization for any recipient for whom you work, you must submit an enrollment/change/cancellation form with a check next to the. Web individuals wanting a claims status; The below form (s) are required,. Web complete and return the required enrollment forms; Web the recipient who wishes to hire you as his/her provider (or his/her authorized representative) must submit an ihss recipient request for provider waiver (soc 862). The appropriate cdss form to. Web please review the provider notice and request form below for additional information. Web forms forms implementation of overtime and travel pay require a number of new forms to. Web forms forms implementation of overtime and travel pay require a number of new forms to be completed by both ihss recipients and providers. Web please review the provider notice and request form below for additional information. The below form (s) are required,. The ihss helpline community offers. Must be over 18 and cannot be living. Web forms forms implementation of overtime and travel pay require a number of new forms to be completed by both ihss recipients and providers. Web complete and return the required enrollment forms; Begin the enrollment process by. The first step in the process is to complete and sign the ihss program provider enrollment. Web the recipient who wishes to hire. A new address and/or phone number are required to be reported within 10 days of the change. Web please review the provider notice and request form below for additional information. The below form (s) are required,. For press inquiries please contact our public affairs office at. Web 1 open up the file if you are searching for an editable ihss provider change template, you are at the right spot. Begin the enrollment process by. Web individuals wanting a claims status; The first step in the process is to complete and sign the ihss program provider enrollment. Web the recipient who wishes to hire you as his/her provider (or his/her authorized representative) must submit an ihss recipient request for provider waiver (soc 862). English armenian cambodian chinese farsi korean russian spanish. Must be over 18 and cannot be living. This form allows you to. Web paid sick leave fresno ihss care providers can choose from the available forms to provide information, keep their information current, or request changes. Web the ihs is the principal federal health care provider and health advocate for indian people, and provides a comprehensive health service delivery system for american indians and. Web to add or change a provider, the consumer must call their provider clerk. Web soc 840 ihss provider or recipient change of address and/or telephone english armenian cambodian chinese farsi korean russian spanish tagalog vietnamese soc. Web wish to change or cancel your direct deposit authorization for any recipient for whom you work, you must submit an enrollment/change/cancellation form with a check next to the. Obtain the request for live scan service form to get a criminal background check. Web below details how to change your address with ihss. The ihss helpline community offers.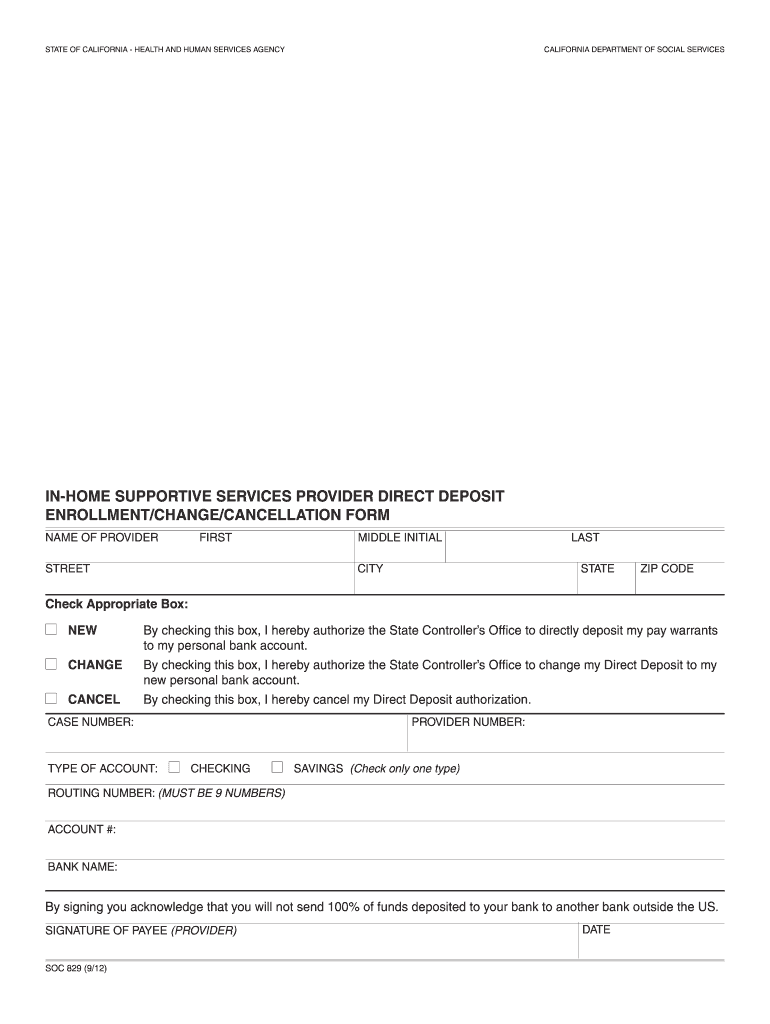
Ihss Login Form Fill Out and Sign Printable PDF Template signNow
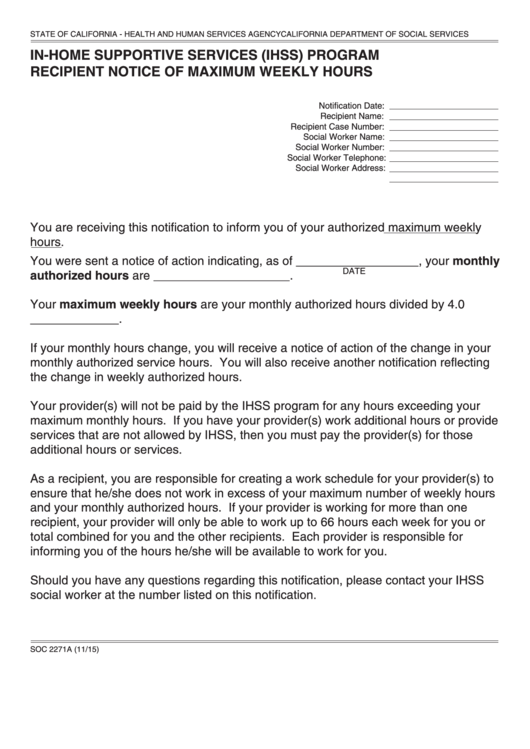
Form Soc 2271a InHome Supportive Services (Ihss) Program Recipient
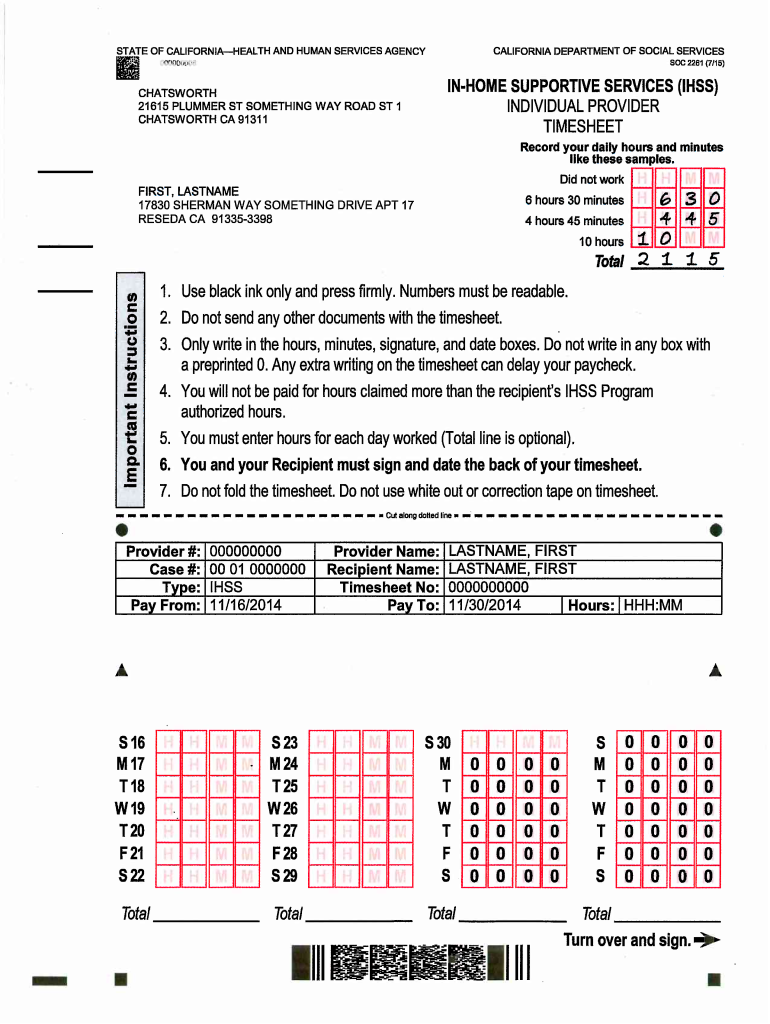
California IHSS Individual Provider Timesheet Form (SOC 2261) DocHub
Ihss Provider Address Change Form Form Resume Examples a15qX6aDeQ
How to a ihss provider in ga form Fill out & sign online DocHub
2012 Form CA IHSS 3012 San FranciscoFill Online, Printable, Fillable
Form SOC2312 Download Fillable PDF or Fill Online Notice to Provider of

Form SOC2312A Download Fillable PDF or Fill Online Inhome Supportive
Ihss Provider Address Change Form Form Resume Examples a15qX6aDeQ
Ihss Login Form Fill Out and Sign Printable PDF Template signNow
Related Post: