Highmark Bcbs Prior Authorization Form
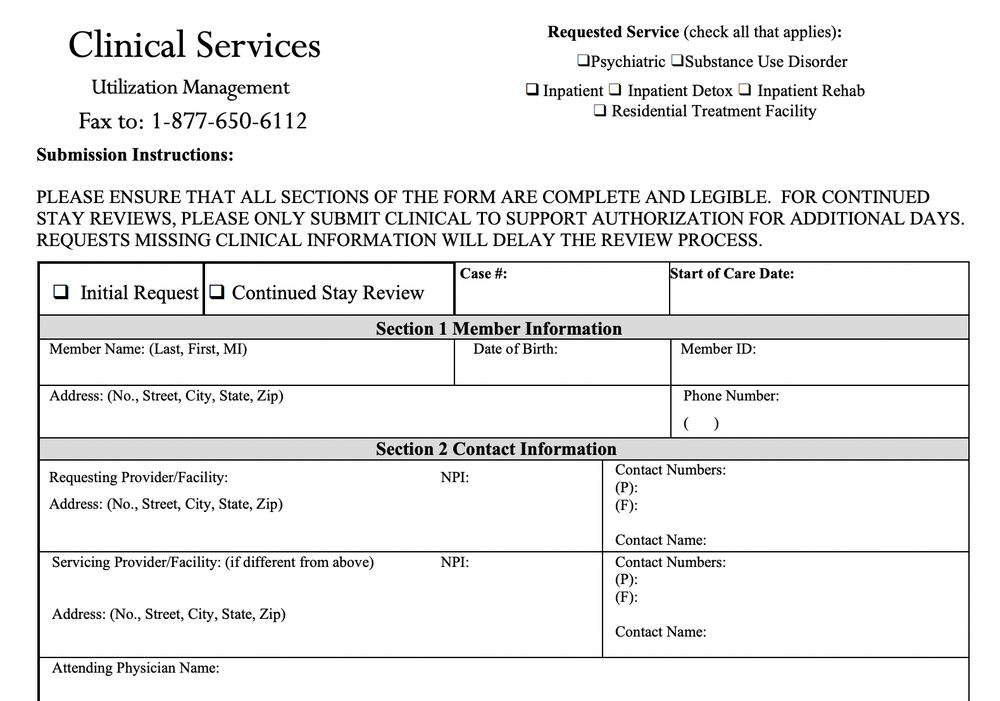
Highmark Bcbs Prior Authorization Form - However, if your employer purchased your plan before the affordable care act was enacted, you may. Web we can also give you information in a different language. Submit a separate form for each medication. Complete and fax all requested information below including any supporting documentation as applicable to highmark health. Web prior authorization for the following drugs and/or therapeutic categories, the diagnosis, applicable lab data, and involvement of specialists are required, plus additional. Web pharmacy prior authorization forms addyi prior authorization form armodafinil prior authorization form blood disorders medication request form cgrp inhibitors. Web medicare part d hospice prior authorization information. Web independent blue cross blue shield plans. Web outpatient therapy services prior authorization request form use this form for all physical, occupational, speech, and feeding therapies, pulmonary and cardiac. Complete all information on the form. Web pharmacy prior authorization forms addyi prior authorization form armodafinil prior authorization form blood disorders medication request form cgrp inhibitors. Any service that requires an authorization from a primary payer, except nonexhausted original medicare services. Complete and fax all requested information below including any supporting documentation as applicable to. Complete all information on the form. Highmark blue cross blue shield,. Web to search for a specific procedure code on the list of procedures/dme requiring authorization, press control key + f key, enter the procedure code and press enter. Designation of personal representative for appeal process; Web durable medical equipment (dme) prior authorization request form. Note:the prescribing physician (pcp or specialist) should, in most cases, complete the. Complete all information on. Use this form to request coverage/prior authorization of medications for individuals in hospice care. Web medicare part d hospice prior authorization information. Web this information is issued by highmark blue shield on behalf of its affiliated blue companies, which are independent licensees of the blue cross blue shield. Highmark blue cross blue shield, highmark choice company, highmark health insurance company,. Complete all information on the form. Web medicare part d hospice prior authorization information. Web durable medical equipment (dme) prior authorization request form. Web specialty drugs requiring prior authorization for specialty drugs within the therapeutic categories listed below, the diagnosis, applicable lab data, and additional. Highmark blue cross blue shield, highmark choice company, highmark health insurance company, highmark coverage advantage,. Web for a complete list of services requiring authorization, please access the authorization requirements page on the highmark provider resource center under claims, payment. Web durable medical equipment (dme) prior authorization request form. Testosterone product prior authorization form. Web this information is issued by highmark blue shield on behalf of its affiliated blue companies, which are independent licensees of the. Web specialty drugs requiring prior authorization for specialty drugs within the therapeutic categories listed below, the diagnosis, applicable lab data, and additional. Web for a complete list of services requiring authorization, please access the authorization requirements page on the highmark provider resource center under claims, payment. Designation of personal representative for appeal process; Complete all information on the form. Web. Web for a complete list of services requiring authorization, please access the authorization requirements page on the highmark provider resource center under claims, payment. However, if your employer purchased your plan before the affordable care act was enacted, you may. Web outpatient therapy services prior authorization request form use this form for all physical, occupational, speech, and feeding therapies, pulmonary. Web pharmacy prior authorization forms addyi prior authorization form armodafinil prior authorization form blood disorders medication request form cgrp inhibitors. Use this form to request coverage/prior authorization of medications for individuals in hospice care. Complete and fax all requested information below including any supporting documentation as applicable to highmark health. Web prior authorization for the following drugs and/or therapeutic categories,. Web to search for a specific procedure code on the list of procedures/dme requiring authorization, press control key + f key, enter the procedure code and press enter. Web prior authorization for the following drugs and/or therapeutic categories, the diagnosis, applicable lab data, and involvement of specialists are required, plus additional. Any service that requires an authorization from a primary. Web medicare part d hospice prior authorization information. Web highmark expanding our prior authorization requirements. Complete all information on the form. Designation of personal representative for appeal process; Complete and fax all requested information below including any supporting documentation as applicable to. Web for other helpful information, please visit the highmark web site at: Any service that requires an authorization from a primary payer, except nonexhausted original medicare services. Designation of personal representative for appeal process; Complete all information on the form. Web to search for a specific procedure code on the list of procedures/dme requiring authorization, press control key + f key, enter the procedure code and press enter. Submit a separate form for each medication. Web outpatient therapy services prior authorization request form use this form for all physical, occupational, speech, and feeding therapies, pulmonary and cardiac. Web pharmacy prior authorization forms addyi prior authorization form armodafinil prior authorization form blood disorders medication request form cgrp inhibitors. Highmark blue cross blue shield, highmark choice company, highmark health insurance company, highmark coverage advantage,. Web we can also give you information in a different language. Web durable medical equipment (dme) prior authorization request form. Web for a complete list of services requiring authorization, please access the authorization requirements page on the highmark provider resource center under claims, payment. Web medicare part d hospice prior authorization information. Web highmark expanding our prior authorization requirements. Web specialty drugs requiring prior authorization for specialty drugs within the therapeutic categories listed below, the diagnosis, applicable lab data, and additional. However, if your employer purchased your plan before the affordable care act was enacted, you may. Testosterone product prior authorization form. Complete and fax all requested information below including any supporting documentation as applicable to highmark health. Note:the prescribing physician (pcp or specialist) should, in most cases, complete the. Web this information is issued by highmark blue shield on behalf of its affiliated blue companies, which are independent licensees of the blue cross blue shield.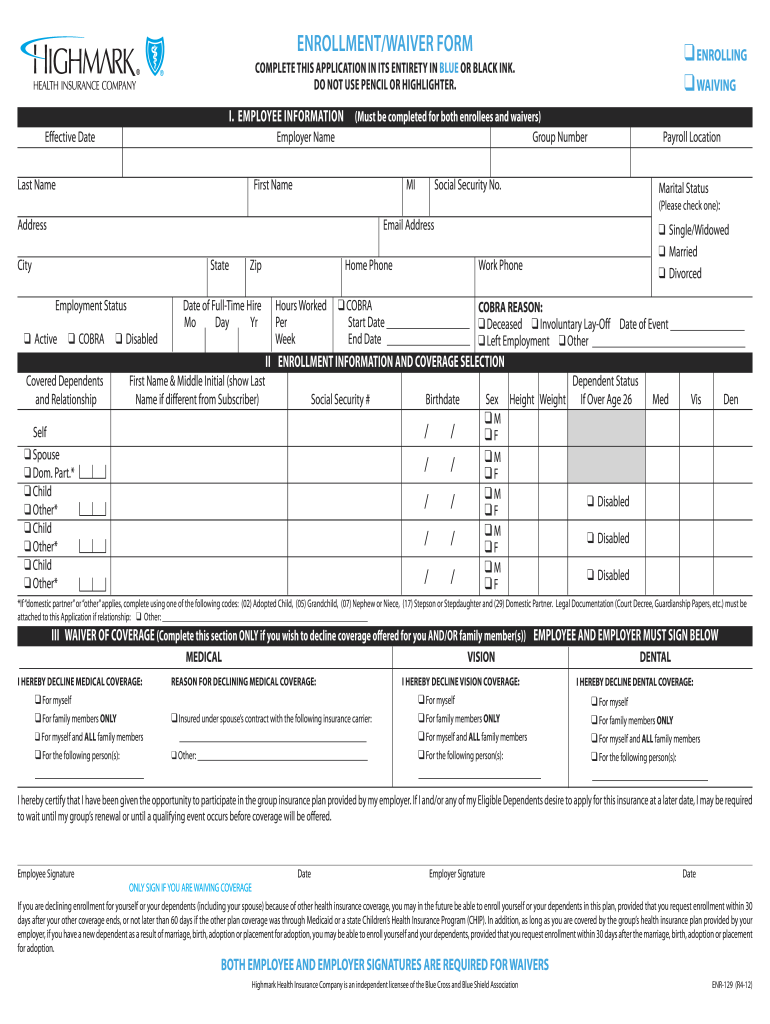
Highmark enrollment form Fill out & sign online DocHub
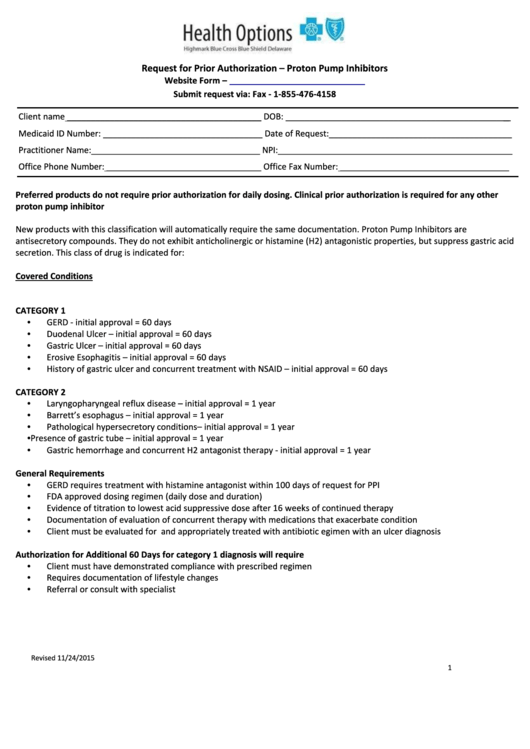
Request For Prior Authorization Form Proton Pump Inhibitors
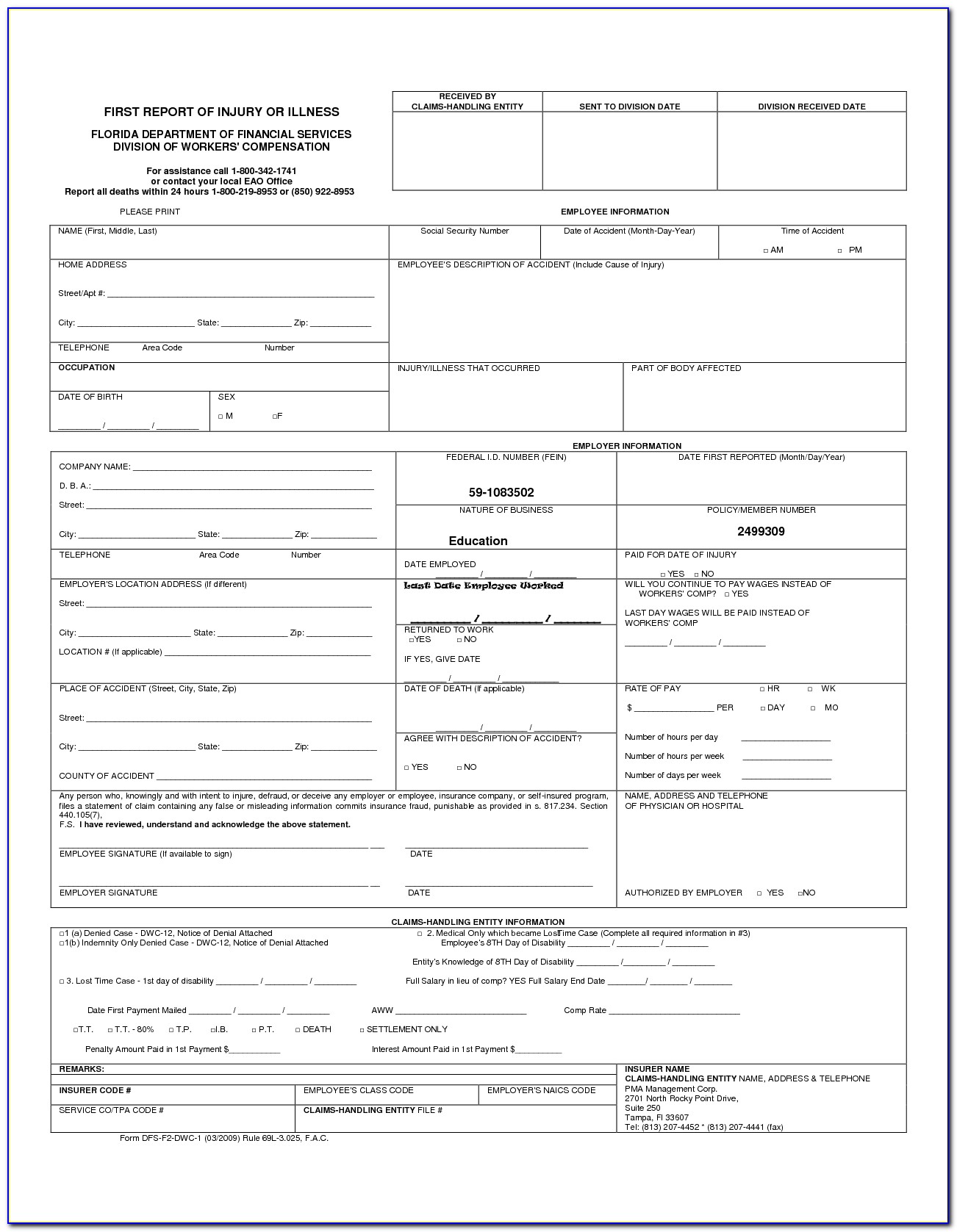
Bcbs Prior Auth Forms Florida Form Resume Examples A4kn4J95jG
Bcbs Kansas City Prior Authorization Form Fill Out and Sign Printable
Form ENR187 Download Printable PDF or Fill Online Disabled Child
Highmark BCBS CLM038 2000 Fill and Sign Printable Template Online

Free Highmark Prior (Rx) Authorization Form PDF eForms

Free Prior (Rx) Authorization Forms PDF eForms
Highmark bcbs authorization form
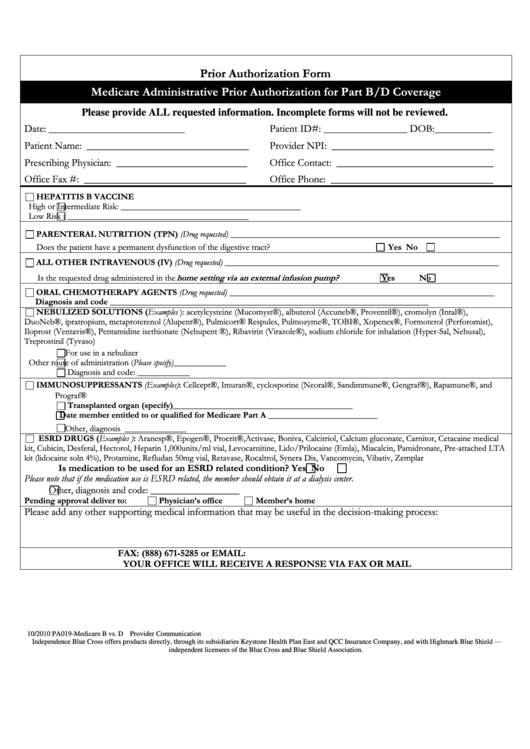
Medicare Administrative Prior Authorization For Part B/d Coverage
Related Post: