Form Omb 0938
Form Omb 0938 - We need the following information regarding the above. Web application for enrollment in medicare part b (medical insurance) department of health and human services centers for medicare &. You must specify the applicable calendar year or tax year to which your. Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. What is the purpose of this form? Select the document you want to sign and click upload. Web how you can complete the omb no 0938 0086 form on the internet: To sign up for part b in one of these situations, you’ll also need to fill out and submit an application for enrollment in. Guidance for advance beneficiary notice of non. To start the document, utilize the fill camp; Web attach form 8938 to your annual return and file by the due date (including extensions) for that return. Web form approved (x2) multiple construction b. Web how you can complete the omb no 0938 0086 form on the internet: Application for medicare part a and part b special enrollment period (exceptional circumstances) form and instruction. Authorization to disclose personal. Application for medicare part a and part b special enrollment period (exceptional circumstances) form and instruction. Department of health and human services centers for medicare & medicaid services. Sign online button or tick the preview image of the form. The information collected on the form is needed to. In order to apply for medicare in a special. Web how you can complete the omb no 0938 0086 form on the internet: Web form approved (x2) multiple construction b. Centers for medicare & medicaid services. What is the purpose of this form? Web request for employment information. Application for medicare part a and part b special enrollment period (exceptional circumstances) form and instruction. Web request for employment information. Wing _____ department of health and human services centers for medicare & medicaid services omb no. Department of health and human services centers for medicare & medicaid services. Web application for enrollment in medicare part b (medical insurance) department. Department of health and human services centers for medicare & medicaid services. In order to apply for medicare in a special. Emergency and foreign hospital services beneficiary statement in canadian/mexican. To start the document, utilize the fill camp; Web attach form 8938 to your annual return and file by the due date (including extensions) for that return. You must specify the applicable calendar year or tax year to which your. Web attach form 8938 to your annual return and file by the due date (including extensions) for that return. Web application for enrollment in medicare part b (medical insurance) department of health and human services centers for medicare &. • you must make your request to the. Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. Web how you can complete the omb no 0938 0086 form on the internet: Web application for enrollment in medicare part b (medical insurance) department of health and human services centers for medicare &. Web attach form 8938 to your annual return and file by. Web form approved (x2) multiple construction b. Web form approved omb no. Department of health and human services centers for medicare & medicaid services. Web request for employment information. Application for medicare part a and part b special enrollment period (exceptional circumstances) form and instruction. Emergency and foreign hospital services beneficiary statement in canadian/mexican. Web how you can complete the omb no 0938 0086 form on the internet: Centers for medicare & medicaid services. Web attach form 8938 to your annual return and file by the due date (including extensions) for that return. Web request for employment information. What is the purpose of this form? In order to apply for. Emergency and foreign hospital services beneficiary statement in canadian/mexican. This paperwork package provides information regarding the form used by the medicare,. Centers for medicare & medicaid services. To start the document, utilize the fill camp; In order to apply for. What is the purpose of this form? Web attach form 8938 to your annual return and file by the due date (including extensions) for that return. What is the purpose of this form? We need the following information regarding the above. Web form approved omb no. How to ask for an appeal of your hospital discharge. Web how you can complete the omb no 0938 0086 form on the internet: The information collected on the form is needed to. • you must make your request to the qio listed. To sign up for part b in one of these situations, you’ll also need to fill out and submit an application for enrollment in. Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. Web form approved omb no. Wing _____ department of health and human services centers for medicare & medicaid services omb no. Guidance for advance beneficiary notice of non. Select the document you want to sign and click upload. Web request for employment information. 11/30/2023) • plans may provide a brief description of any medicare or medicaid coverage rule or plan policy included in the. Department of health and human services centers for medicare & medicaid services.
Fillable Online Form Approved OMB No. 09380679 02/2024 CERTIFICATE OF
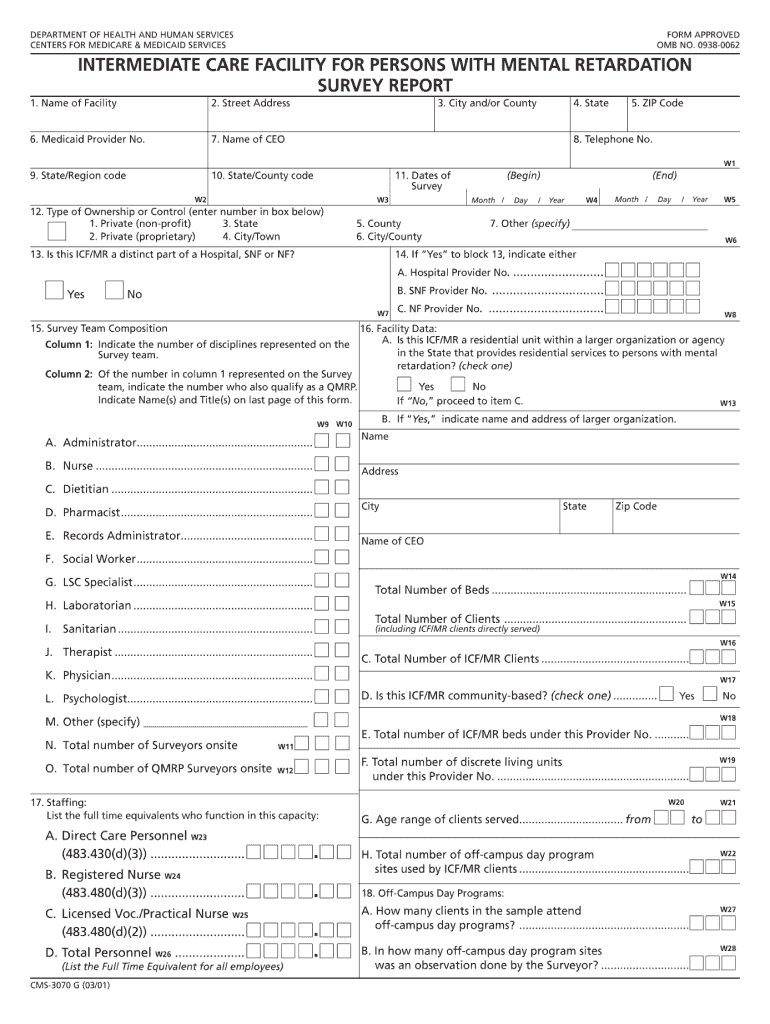
OMB No 0938 0062 Form Fill Out and Sign Printable PDF Template signNow

OMB No. 09380357 HOME HEALTH CERTIFICATION Approved OMB No. 09380357
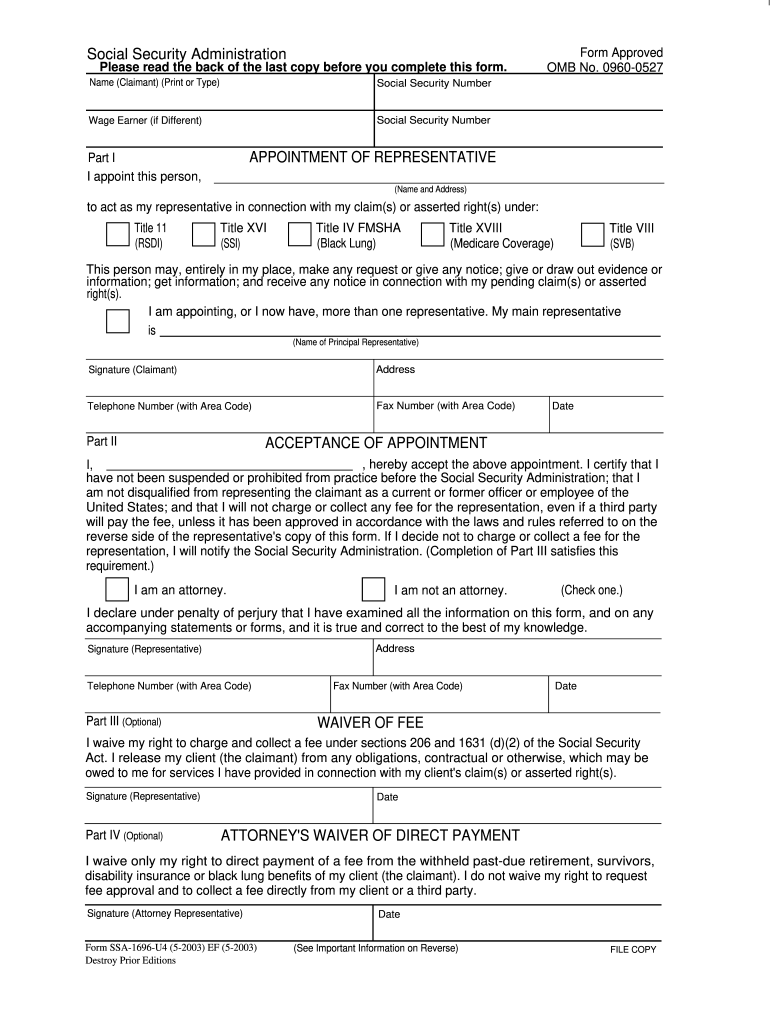
Social Security Form Omb No 09380787 Printable

Fillable Online OMB No. 09381378 Expires7/31/2023 Who can use this

Fillable Online omb0938 0214 1990 form Fax Email Print pdfFiller

Form Approved Omb No 0938 0787 Fill Online, Printable, Fillable
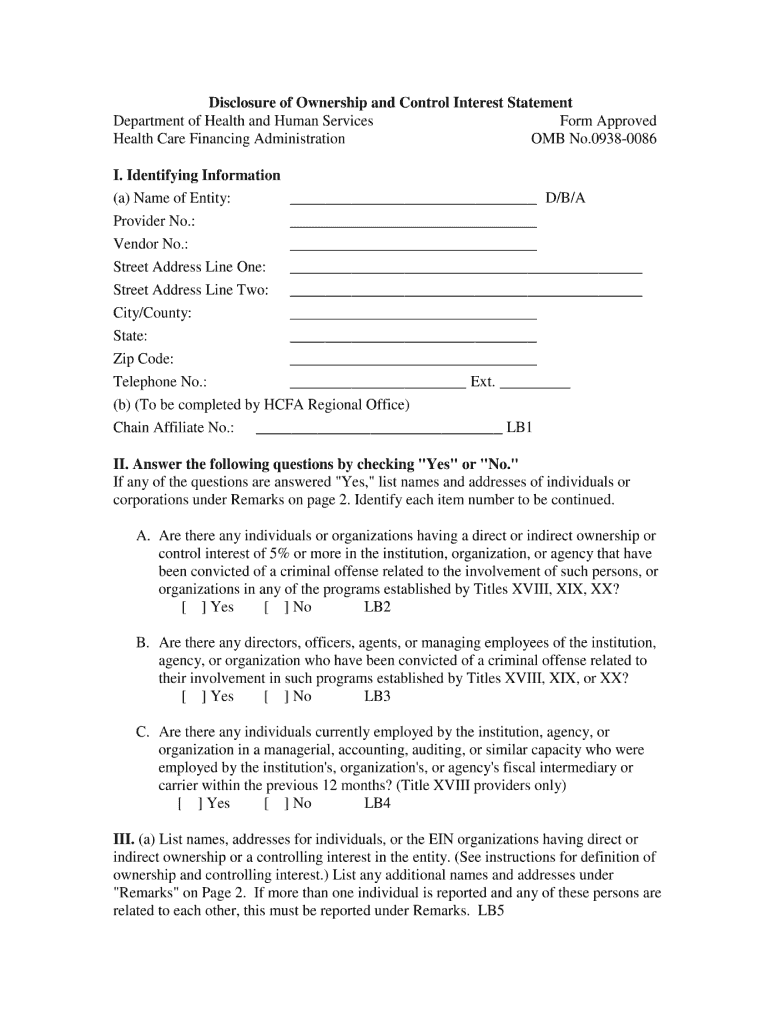
Omb 0938 Interest Form Fill Online, Printable, Fillable, Blank

NPI NPI ICE npi npi npi npi npi approved by national uniform claim

New 2500 CMS 1500 Claim Forms Current HCFA 02/2012
Related Post: