Florida Medicaid Appeal Form
Florida Medicaid Appeal Form - Grievance/appeal request form—spanish (157 kb),. If the plan’s decision is not in your favor, you can request a medicaid fair hearing you can ask for a fair hearing by. Web if we deny the request for a fast appeal, we will transfer the appeal into the regular appeal time frame of 30 days. Appeals must be submitted using the following. Web the florida agency for persons with disabilities (apd) offers two types of administrative hearings to individuals substantially affected by actions of the agency. Web florida medicaid authorization requirements are authorized by the following: Grievance/appeal request form—english (157 kb), pdf. Ad compare all your options at medicare.gov, the official source for medicare information. Web part b appeals forms providers, participating physicians, and other suppliers have the right to appeal claim decisions. Web we can help you write your appeal. Web the florida agency for persons with disabilities (apd) offers two types of administrative hearings to individuals substantially affected by actions of the agency. It is on the front of your member id. Web download and return to us the completed forms: Grievance/appeal request form—spanish (157 kb),. Web to submit a complaint online you may use the florida medicaid complaint. You can also request a review by the state by: The health plan must resolve a plan appeal. Web part b appeals forms providers, participating physicians, and other suppliers have the right to appeal claim decisions. Signnow allows users to edit, sign, fill and share all type of documents online. Ad register and subscribe now to work on your wellcare. Web if we deny the request for a fast appeal, we will transfer the appeal into the regular appeal time frame of 30 days. Web this letter is called a notice of plan appeal resolution. Web whether you or other household members who were terminated might still be eligible for medicaid and whether an appeal is appropriate or you can. Web you can ask for an expedited appeal if you think waiting up to 30 days is harmful to your health. How do health care providers and health plans contact the statewide provider and health plan claim dispute resolution program (maximus)? If the plan’s decision is not in your favor, you can request a medicaid fair hearing you can ask. Web this letter is called a notice of plan appeal resolution. How do health care providers and health plans contact the statewide provider and health plan claim dispute resolution program (maximus)? Appeals must be submitted using the following. Your first and last name ; Web children's medical services (cms) health plan provider manual (pdf) medicaid provider billing manual (pdf) forms. It is on the front of your member id. If you disagree with our decision to deny a fast appeal, call us to. Web if we deny the request for a fast appeal, we will transfer the appeal into the regular appeal time frame of 30 days. Signnow allows users to edit, sign, fill and share all type of documents. Web part b appeals forms providers, participating physicians, and other suppliers have the right to appeal claim decisions. Web florida medicaid authorization requirements are authorized by the following: Find the right plan for you. Web you can ask for an expedited appeal if you think waiting up to 30 days is harmful to your health. Ad register and subscribe now. Grievance/appeal request form—spanish (157 kb),. Signnow allows users to edit, sign, fill and share all type of documents online. Web download and return to us the completed forms: Web if you aren’t satisfied with the outcome of a claim reconsideration request, you may submit a formal claim dispute/appeal using the process outlined in your care provider manual. Web we can. Web if you aren’t satisfied with the outcome of a claim reconsideration request, you may submit a formal claim dispute/appeal using the process outlined in your care provider manual. Web with the end of the emergency, the state began redeterminations, and the medicaid rolls had dropped to about 5.25 million in august, according to the state. Web formal claim appeal. Grievance/appeal request form—spanish (157 kb),. Please refer to the new provider complaint tip sheet [ 282.6 kb ] for helpful hints on submitting. Web florida medicaid authorization requirements are authorized by the following: Print the form, complete it and mail or fax it to a. Find the right plan for you. Web the florida agency for persons with disabilities (apd) offers two types of administrative hearings to individuals substantially affected by actions of the agency. How to request an expedited appeal you can request an expedited appeal. The health plan must resolve a plan appeal. Print the form, complete it and mail or fax it to a. Web formal claim appeal request. Use this form to request a formal claim appeal. Web to submit a complaint online you may use the florida medicaid complaint form. Find the right plan for you. Ad register and subscribe now to work on your wellcare provider payment dispute request form. Web florida medicaid forms adopted rules florida medicaid forms form number form name effective date ahca medserv form 004 part a preadmission screen and. Web application forms and instructions on how to file claims disputes can be obtained directly from maximus by calling. Web if we deny the request for a fast appeal, we will transfer the appeal into the regular appeal time frame of 30 days. Web a plan appeal is when the enrollee disagrees with the health plan’s adverse benefit determination and wants to seek a review. Web part b appeals forms providers, participating physicians, and other suppliers have the right to appeal claim decisions. How do health care providers and health plans contact the statewide provider and health plan claim dispute resolution program (maximus)? Appeals must be submitted using the following. If you disagree with our decision to deny a fast appeal, call us to. Web if you aren’t satisfied with the outcome of a claim reconsideration request, you may submit a formal claim dispute/appeal using the process outlined in your care provider manual. Use this form to submit adjustment s/voids, to. Web children's medical services (cms) health plan provider manual (pdf) medicaid provider billing manual (pdf) forms provider dispute form (pdf) provider claim adjustment.
Medi Cal Appeal Form 90 1 Pdf Fill Online, Printable, Fillable, Blank
Fillable Florida Medicaid Prior Authorization printable pdf download
Notice of Appeal Florida Sample Form Fill Out and Sign Printable PDF
Wellcare Appeal Form Pdf Fill Online, Printable, Fillable, Blank
Form DEOA100(E) Download Printable PDF or Fill Online Notice of Appeal

Medicare Appeal Letter SampleTemplatess SampleTemplatess
Sample Medicaid Appeal Letter Download Printable PDF Templateroller
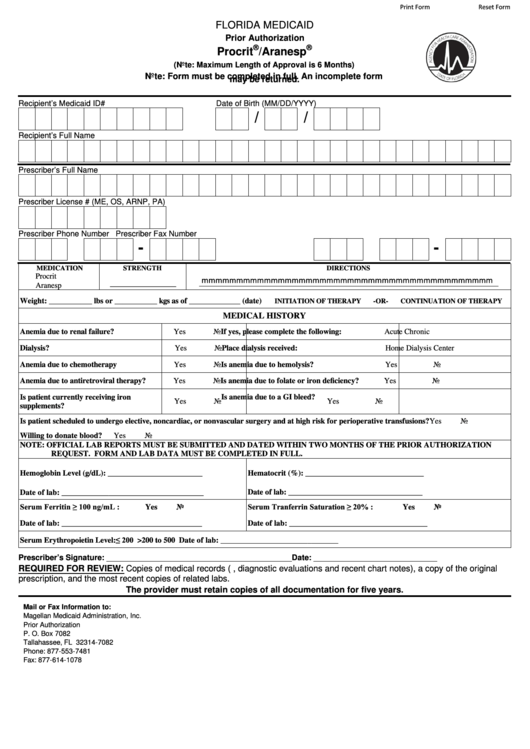
Fillable Prior Authorization Form Procrit/aranespFlorida Medicaid
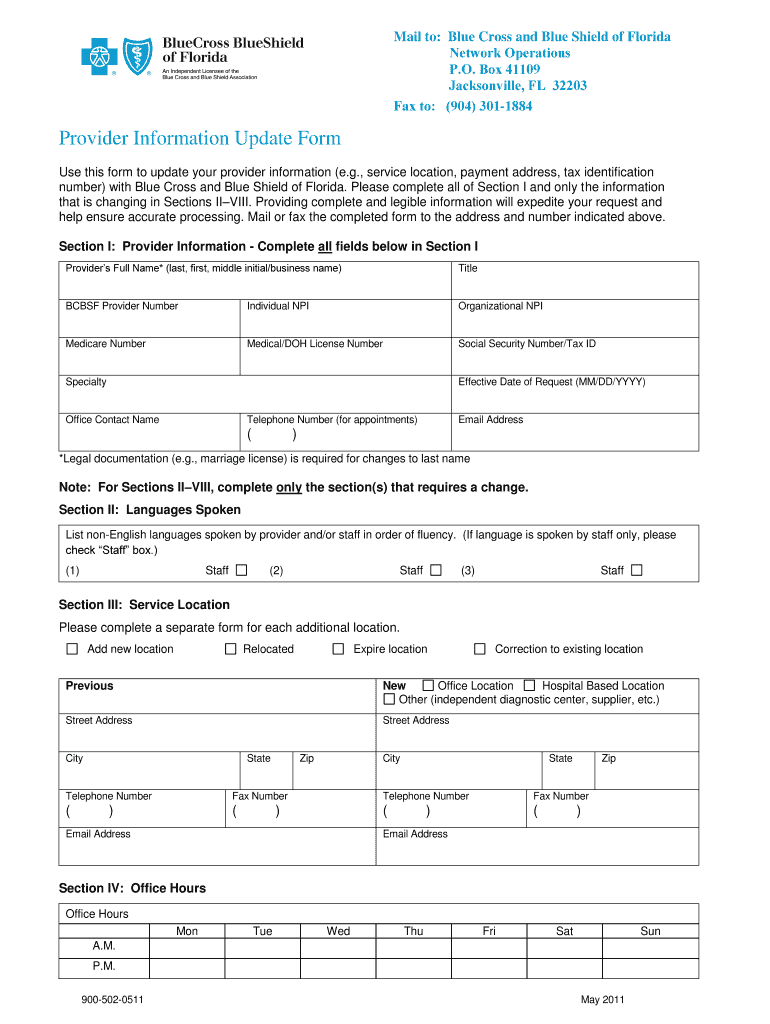
Florida Blueshield Provider Form Fill Online, Printable, Fillable
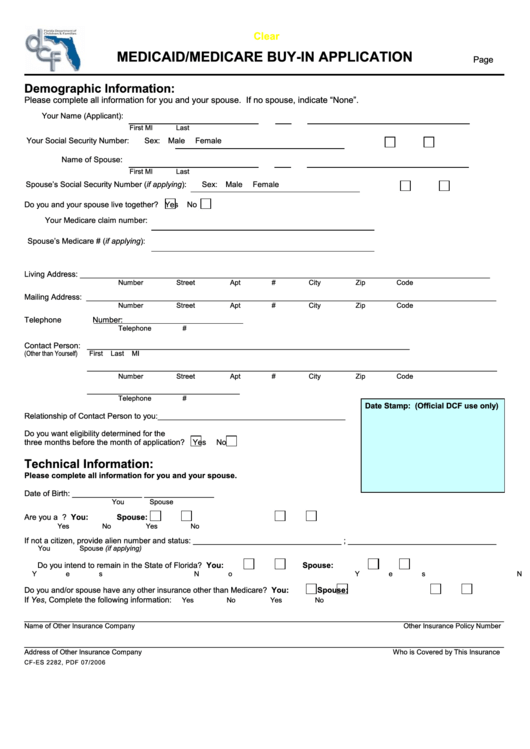
Fillable Florida Medicaid/medicare BuyIn Application Form printable
Related Post: