Dwc Rfa Form
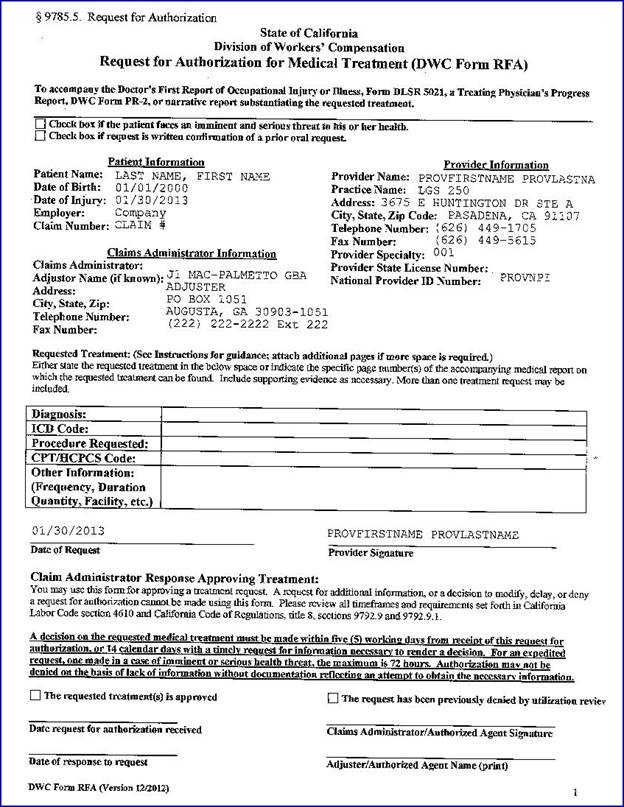
Dwc Rfa Form - Web an updated form for the state of california division of workers' compensation request for authorization for medical treatment (a.k.a. Get your online template and fill it in using progressive features. The request for authorization for medical treatment (dwc form rfa) is required for the employee’s treating physician to initiate the utilization review process. If you don’t submit the rfa with the visit. If the request is to continue a treatment plan or therapy, attach. Web use the dwc request for authorization form. Identify both the employee and yourself, identify specifically the recommended treatment or treatments, provide documentation. If the patient is “permanent. Web (a) the request for authorization for a course of treatment as defined in section 9792.6.1(d) must be in written form set forth on the “request for authorization (dwc form rfa),”. This form must accompany the doctor’s first report of occupational injury or illness, form dlsr 5021,. The dwc form rfa must contain all the information needed to substantiate the request for authorization. This form must accompany the doctor’s first report of occupational injury or illness, form dlsr 5021,. Web request for authorization for medical treatment (dwc form rfa) to accompany the doctor’s first report of occupational injury or illness, form dlsr 5021, a treating. Web (a). Web the request for authorization for medical treatment (dwc form rfa) is required for the employee’s treating physician to initiate the utilization review process required by labor. Web the dwc form rfa and reports must contain all the information needed to substantiate the request for authorization. Enjoy smart fillable fields and interactivity. Web request for authorization for medical treatment (dwc. If the patient is “permanent. Web dwc public records office division of workers' compensation p.o. If the request is to continue a treatment plan or therapy, attach. This form must accompany the doctor’s first report of occupational injury or illness, form dlsr 5021,. Web the request for authorization for medical treatment (dwc form rfa) is required for the employee’s treating. Web an updated form for the state of california division of workers' compensation request for authorization for medical treatment (a.k.a. This form must accompany the doctor’s first report of occupational injury or illness, form dlsr 5021,. If the request is to continue a treatment plan or therapy, attach. Web the request for authorization for medical treatment (dwc form rfa) is. Web dwc form rfa, or a request for authorization accepted as complete under section 9792.9.1(c)(2), is first received by the claims administrator, or in the case of prior. Web the request for authorization for medical treatment (dwc form rfa) is required for the employee’s treating physician to initiate the utilization review process required by labor. Web dwc public records office. Periodic report (required 45 days after last report) change in treatment plan release from care change in work status need for. Web request for authorization for medical treatment (dwc form rfa) to accompany the doctor’s first report of occupational injury or illness, form dlsr 5021, a treating. Web use the dwc request for authorization form. Web the dwc form rfa. Web the request for authorization for medical treatment (dwc form rfa) is required for the employee’s treating physician to initiate the utilization review process required by labor. The dwc form rfa must contain all the information needed to substantiate the request for authorization. List the requested treatment, the purpose of the treatment. Web request for authorization for medical treatment (dwc. Periodic report (required 45 days after last report) change in treatment plan release from care change in work status need for. This form must accompany the doctor’s first report of occupational injury or illness, form dlsr 5021,. Web request for authorization for medical treatment (dwc form rfa) to accompany the doctor’s first report of occupational injury or illness, form dlsr. Web dwc public records office division of workers' compensation p.o. Web how to fill out and sign dwc form rfa online? Get your online template and fill it in using progressive features. If the patient is “permanent. List the requested treatment, the purpose of the treatment. Web how to fill out and sign dwc form rfa online? Web dwc public records office division of workers' compensation p.o. Periodic report (required 45 days after last report) change in treatment plan release from care change in work status need for. The request for authorization for medical treatment (dwc form rfa) is required for the employee’s treating physician to. Web an updated form for the state of california division of workers' compensation request for authorization for medical treatment (a.k.a. The dwc form rfa must contain all the information needed to substantiate the request for authorization. If the request is to continue a treatment plan or therapy, attach. List the requested treatment, the purpose of the treatment. Web use the dwc request for authorization form. Web request for authorization for medical treatment (dwc form rfa) to accompany the doctor’s first report of occupational injury or illness, form dlsr 5021, a treating. The request for authorization for medical treatment (dwc form rfa) is required for the employee’s treating physician to initiate the utilization review process. If you don’t submit the rfa with the visit. The request for authorization for medical treatment (dwc form rfa) is required for the employee’s treating physician to initiate the utilization review process. Get your online template and fill it in using progressive features. Web dwc form rfa, or a request for authorization accepted as complete under section 9792.9.1(c)(2), is first received by the claims administrator, or in the case of prior. This form must accompany the doctor’s first report of occupational injury or illness, form dlsr 5021,. Web (a) the request for authorization for a course of treatment as defined in section 9792.6.1(d) must be in written form set forth on the “request for authorization (dwc form rfa),”. If the patient is “permanent. Web request for authorization number form: Web the dwc form rfa is not a separately reimbursable report under the official medical fee schedule, found at california code of regulations, title 8, section 9789.10 et seq. Web the dwc form rfa and reports must contain all the information needed to substantiate the request for authorization. Web how to fill out and sign dwc form rfa online? Web the request for authorization for medical treatment (dwc form rfa) is required for the employee’s treating physician to initiate the utilization review process required by labor. Identify both the employee and yourself, identify specifically the recommended treatment or treatments, provide documentation.
FINAL DWC RFA California Department of Industrial Doc Template
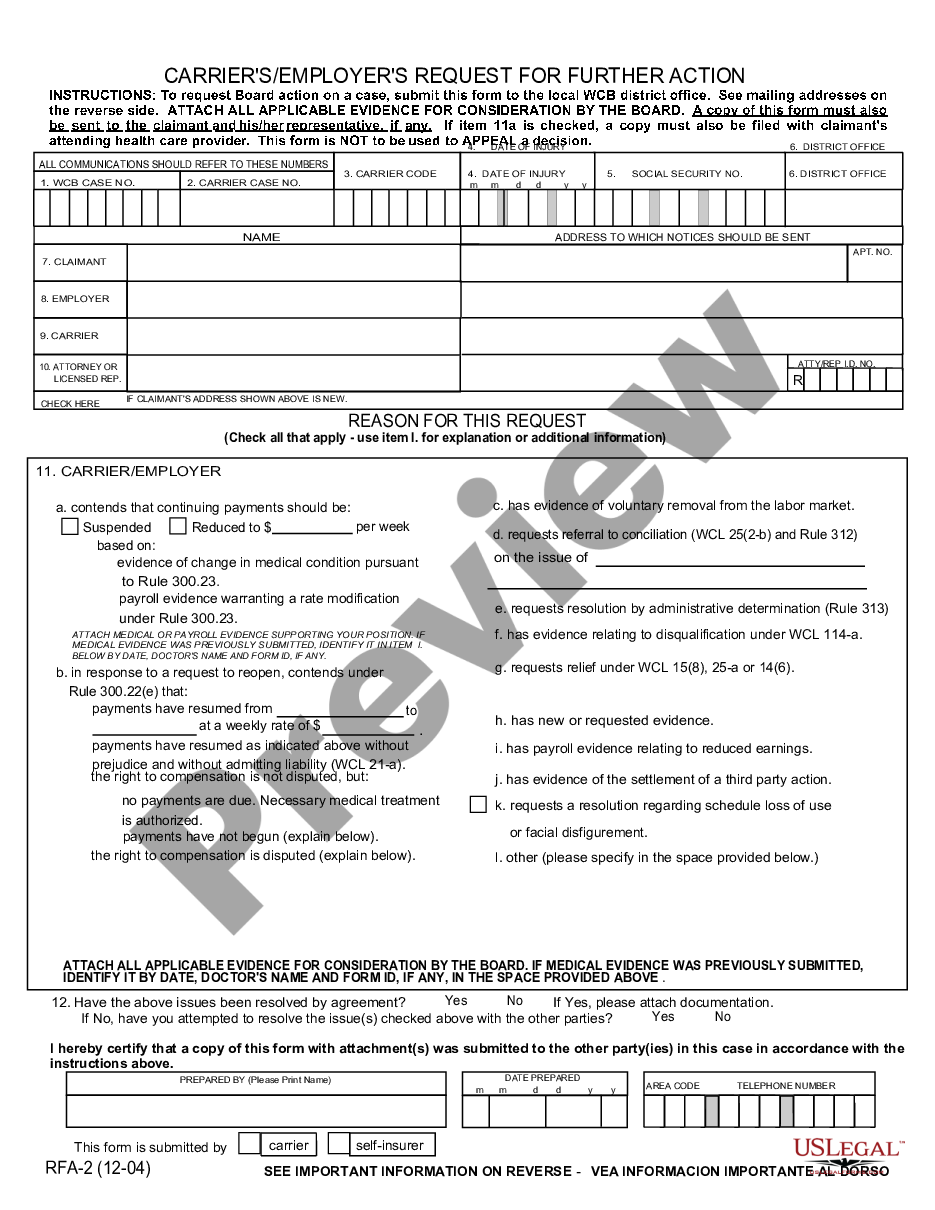
New York Carrier's Employer's Request for Further Action Nys
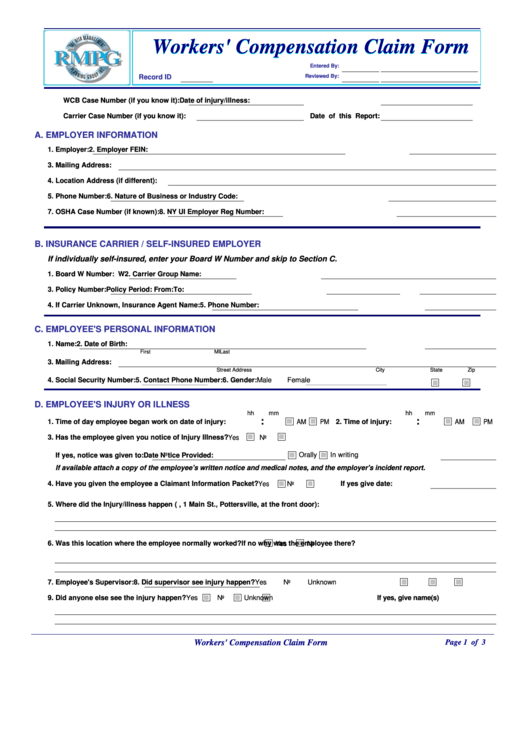
Claim Form Workers Compensation / How to Reduce Workers Compensation

Fillable Online Draft DWC Form033, Request to reduce benefits
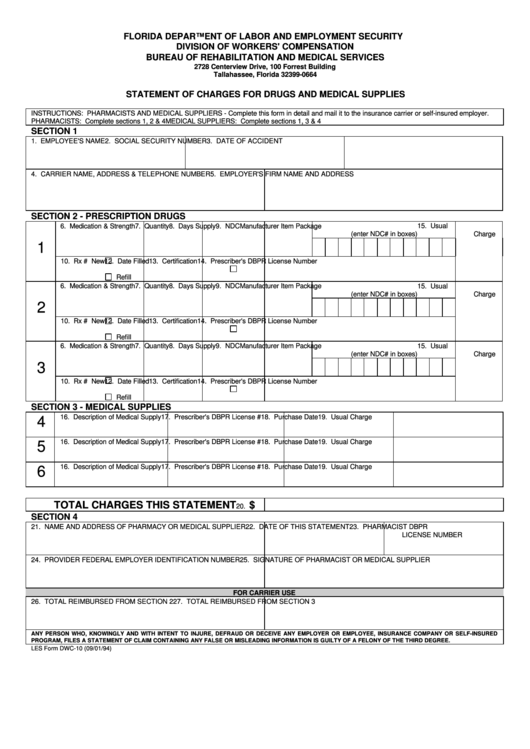
Form Dwc10 Statement Of Charges For Drugs And Medical Supplies
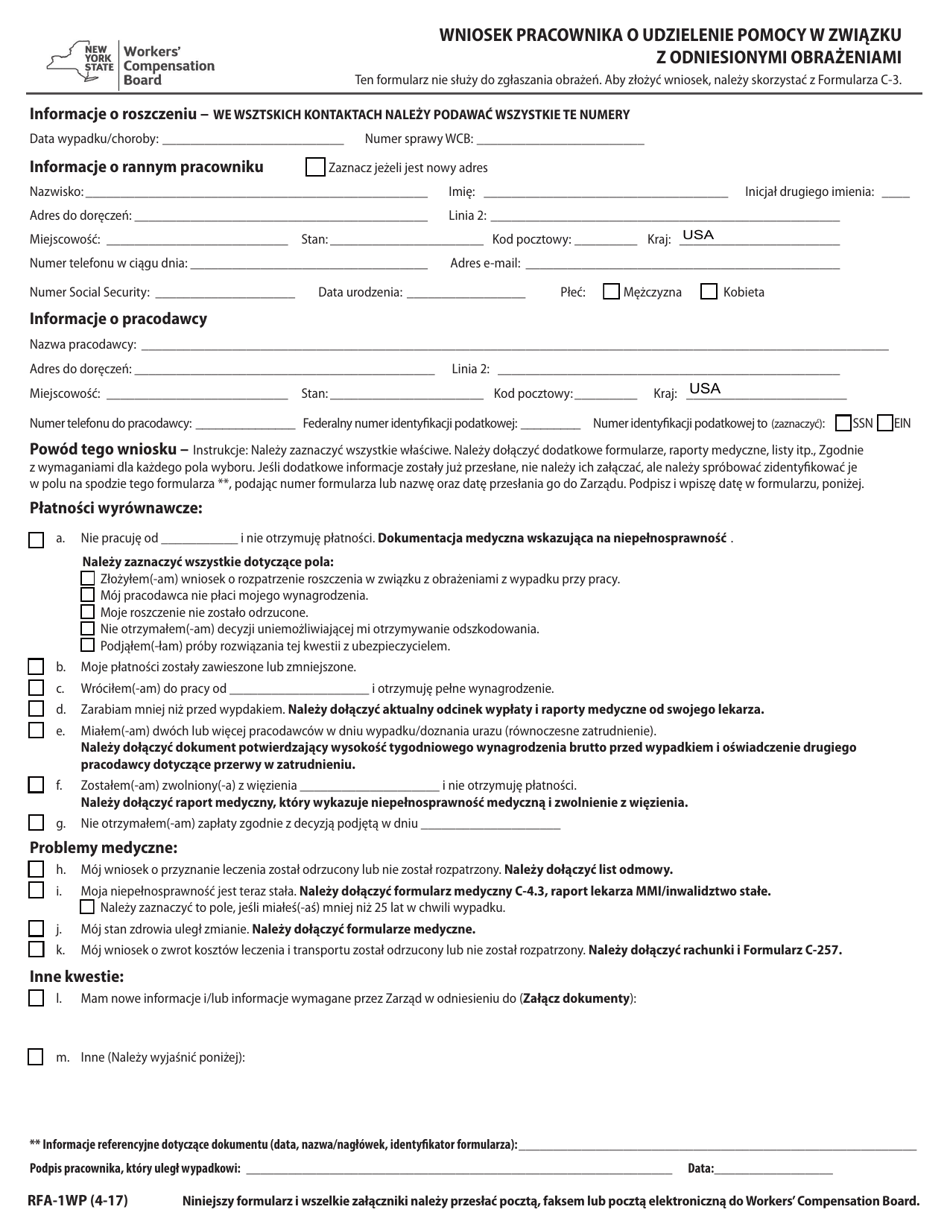
Form RFA1WP Download Fillable PDF or Fill Online Request for

20192022 TX DWC Form73 Fill Online, Printable, Fillable, Blank
Sample DWC Form RFA 122012

CA DWC Form RFA 2014 Fill and Sign Printable Template Online US

Dwc form 003 Fill out & sign online DocHub
Related Post: