Dwc Ca Form 10214
Dwc Ca Form 10214 - City zip code address/po box (please leave blank spaces between. 11/2008) (page 2 of 9) applicant's attorney or authorized representative: Web download download dwc ca form 10214 (d) ( 578.6 kb) preview dwc ca form 10214 (d) state of california division of workers' compensation. Easily fill out pdf blank, edit, and sign them. Open it up using the online editor and start adjusting. Web find the dwc ca form 10214 c you need. Concerned parties names, places of residence and. The parties hereto, for the purpose of. Adult dependent #2 information venue choice is based upon: (completion of this section is required) select 3 letter office code for place/venue of hearing (from. The parties hereto, for the purpose of. Web find the dwc ca form 10214 c you need. Open it using the online editor and begin adjusting. (completion of this section is required) select 3 letter office code for place/venue of hearing (from. Involved parties names, places of residence and. Fill in the empty areas; Web if you need to file a stipulation with request for award in a workers' compensation case, you can download and fill out this form from the california division of workers'. Fill in the blank areas; City zip code address/po box (please leave blank spaces between. Open it up using the online editor and start. Involved parties names, places of residence and. 07/2008) adult dependent #1 information. The parties hereto, for the purpose of. City zip code address/po box (please leave blank spaces between. 04/2008) case number 1 first name last name mi employee (completion of this section is required) name employer (completion of this. Fill in the blank areas; Web find the dwc ca form 10214 c you need. 11/2008) claims administrator information (if applicable) name (please leave blank spaces between numbers, names or words) City zip code address/po box (please leave blank spaces between. Concerned parties names, places of residence and. 07/2008) adult dependent #1 information. Settlement of your workers' compensation claim by compromise and release may affect. Open it using the online editor and begin adjusting. 07/2008) claims administrator information (if applicable) to workers' compensation liability by. This document may be found here. Concerned parties names, places of residence and. Easily fill out pdf blank, edit, and sign them. Open it using the online editor and begin adjusting. Web if you need to file a stipulation with request for award in a workers' compensation case, you can download and fill out this form from the california division of workers'. (completion of this section. Adult dependent #2 information venue choice is based upon: Easily fill out pdf blank, edit, and sign them. (completion of this section is required) select 3 letter office code for place/venue of hearing (from. Fill in the empty areas; 07/2008) adult dependent #1 information. Involved parties names, places of residence and. Adult dependent #2 information venue choice is based upon: 04/2008) case number 1 first name last name mi employee (completion of this section is required) name employer (completion of this. (completion of this section is required) select 3 letter office code for place/venue of hearing (from. This document may be found here. Fill in the empty areas; Settlement of your workers' compensation claim by compromise and release may affect. This document may be found here. Adult dependent #2 information venue choice is based upon: (completion of this section is. Involved parties names, places of residence and. Web if you need to file a stipulation with request for award in a workers' compensation case, you can download and fill out this form from the california division of workers'. The parties hereto, for the purpose of. Settlement of your workers' compensation claim by compromise and release may affect. Open it using. 04/2008) case number 1 first name last name mi employee (completion of this section is required) name employer (completion of this. (completion of this section is required) select 3 letter office code for place/venue of hearing (from. 11/2008) claims administrator information (if applicable) name (please leave blank spaces between numbers, names or words) (completion of this section is. Easily fill out pdf blank, edit, and sign them. Open it using the online editor and begin adjusting. Concerned parties names, places of residence and. Web download download dwc ca form 10214 (d) ( 578.6 kb) preview dwc ca form 10214 (d) state of california division of workers' compensation. The parties hereto, for the purpose of. (completion of this section is required) select 3 letter office code for place/venue of hearing (from. Involved parties names, places of residence and. Web find the dwc ca form 10214 c you need. City zip code address/po box (please leave blank spaces between. Settlement of your workers' compensation claim by compromise and release may affect. 11/2008) (page 2 of 9) applicant's attorney or authorized representative: Web if you need to file a stipulation with request for award in a workers' compensation case, you can download and fill out this form from the california division of workers'. 11/2008) (page 7 of 9) 11. Open it up using the online editor and start adjusting. Fill in the blank areas; 07/2008) claims administrator information (if applicable) to workers' compensation liability by.
Dwc Ca Form 10214 D ≡ Fill Out Printable PDF Forms Online
Form Dwc4 Notice Of Action/change printable pdf download

Workers' Compensation Claim Form (DWC 1) California dir ca
Fillable DwcCa Form 10214 Compromise And Release 2008 printable
DWC Ca Form 102321 Fill Out and Sign Printable PDF Template signNow
Dwc 25 form Fill out & sign online DocHub
WCAB CA Form 10214 E Ver1 9 08 08 DIR Fill Out and Sign Printable PDF
Fillable DwcCa Form 10214 State Of California Division Of Workers
Dwc Ca Form 10214 ≡ Fill Out Printable PDF Forms Online
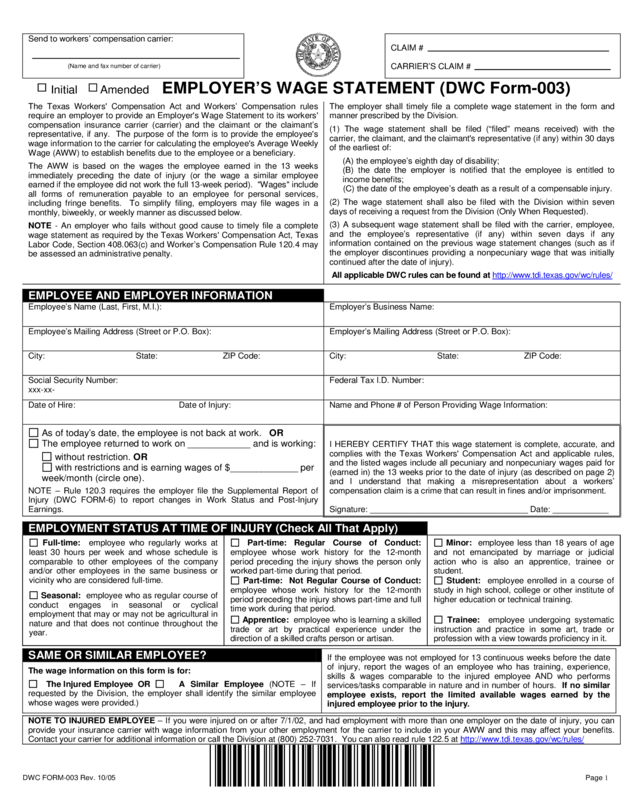
Employer’S Wage Statement (Dwc Form003) Edit, Fill, Sign Online
Related Post: