Ambetter Appeal Form Florida
Ambetter Appeal Form Florida - Web ambetter from coordinated care corporation (04/2021) page 1 ambetter provider reconsiderations, disputes and complaints. Web send a written request by mail to: Web use this form as part of the ambetter from absolute total care request for reconsideration and claim dispute process. Providers, get materials and forms such as the provider manual and commonly used forms. Authorization to disclose health information form. If you choose not to. Web in order to dispute a claim a claim dispute form must be completed and submitted. Web marketplace (ambetter) learn more about sunshine health's practice improvement resource center (pirc) which contains resources such as provider manuals, health. If you wish to file a grievance, appeal, concern or recommendation, please complete this form. Web healthy partnerships are our specialty. Web healthy partnerships are our specialty. To ensure that ambetter member's rights are protected, all ambetter members are entitled to a complaint/grievance and appeals. A request for reconsideration (level i) is. The member can request an appeal within one hundred and eighty (180) calendar days of receipt of a medical necessity denial of medical or behavioral health. Claimsadjustment request &. Request form as cover sheet along with. Web the procedures for filing a complaint/grievance or appeal are outlined in the ambetter member’s evidence of coverage. Web home our health plans show our health plans menu about our plans; Claimsadjustment request & provider claim. Providers, get materials and forms such as the provider manual and commonly used forms. My health pays rewards® ways to save; If you choose not to. Web healthy partnerships are our specialty. You have up to 180 days after date of the denial to request a formal appeal. The member can request an appeal within one hundred and eighty (180) calendar days of receipt of a medical necessity denial of medical or behavioral health. My health pays rewards® ways to save; Claimsadjustment request & provider claim. The member can request an appeal within one hundred and eighty (180) calendar days of receipt of a medical necessity denial of medical or behavioral health. You can count on us to share helpful information. Web use this form as part of the ambetter from absolute total care. Web the procedures for filing a complaint/grievance or appeal are outlined in the ambetter member’s evidence of coverage. Web aetna better health® of florida. My health pays rewards® ways to save; A member may file an appeal orally. Authorization to disclose health information form. Web grievance, appeal, concern or recommendation form. This is the first step in the process if you are an individual and family plan member. My health pays rewards® ways to save; Web ambetter from coordinated care corporation (04/2021) page 1 ambetter provider reconsiderations, disputes and complaints. The member can request an appeal within one hundred and eighty (180) calendar days. Web healthy partnerships are our specialty. Authorization to disclose health information form. With ambetter health, you can rely on the services and support that you need to deliver the best quality of patient care. Web ambetter value plan information. The completed form or your letter should be mailed to:. You have up to 180 days after date of the denial to request a formal appeal. This is the first step in the process if you are an individual and family plan member. You can count on us to share helpful information. Web aetna better health® of florida. If you choose not to. This is the first step in the process if you are an individual and family plan member. Web ambetter from coordinated care corporation (04/2021) page 1 ambetter provider reconsiderations, disputes and complaints. Web ambetter value plan information. My health pays rewards® ways to save; If you choose not to complete this form, you may write a letter that includes the. Web members may also request language assistance or help with other issues. Claimsadjustment request & provider claim. Web find all the forms a member might need — right in one place. With ambetter health, you can rely on the services and support that you need to deliver the best quality of patient care. To ensure that ambetter member's rights are. Web aetna better health® of florida. The member can request an appeal within one hundred and eighty (180) calendar days of receipt of a medical necessity denial of medical or behavioral health. Web marketplace (ambetter) learn more about sunshine health's practice improvement resource center (pirc) which contains resources such as provider manuals, health. Web home our health plans show our health plans menu about our plans; Web members may also request language assistance or help with other issues. Web ambetter from coordinated care corporation (04/2021) page 1 ambetter provider reconsiderations, disputes and complaints. To ensure that ambetter member's rights are protected, all ambetter members are entitled to a complaint/grievance and appeals. The claim dispute form can be found at ambetter.sunflowerhealthplan.com under. Web find all the forms a member might need — right in one place. Web ambetter value plan information. My health pays rewards® ways to save; Request form as cover sheet along with. Web grievance, appeal, concern or recommendation form. You have up to 180 days after date of the denial to request a formal appeal. A request for reconsideration (level i) is. This is the first step in the process if you are an individual and family plan member. Web in order to dispute a claim a claim dispute form must be completed and submitted. Authorization to disclose health information form. Web healthy partnerships are our specialty. If you choose not to complete this form, you may write a letter that includes the information requested below.
Form DEOA100(E) Download Printable PDF or Fill Online Notice of Appeal
Notice of Appeal Florida Sample Form Fill Out and Sign Printable PDF
prior authorization form Fill out & sign online DocHub
Florida Order Denying Petition for Injunction for Protection Against
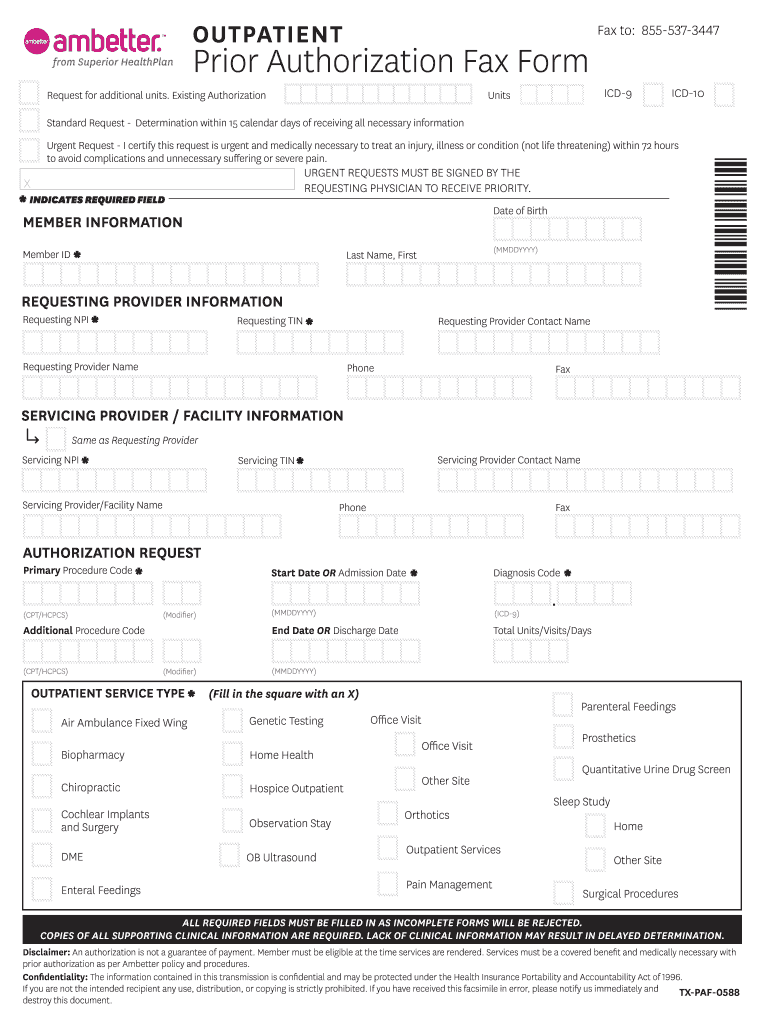
Ambetter Prior Auth Form 2020 Fill and Sign Printable Template Online
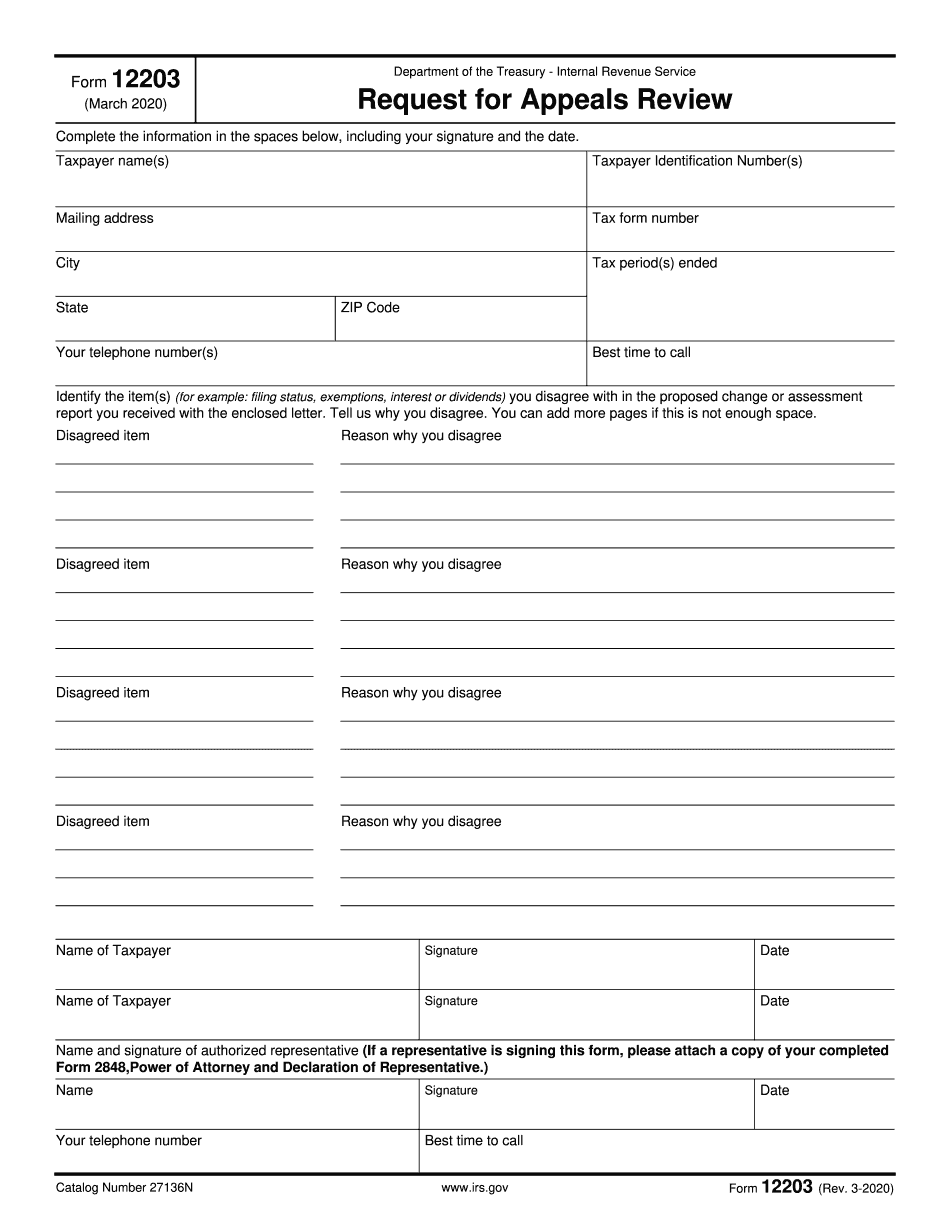
irs appeal form 9423 Fill Online, Printable, Fillable Blank form

Provider Instructions Fill Online, Printable, Fillable, Blank pdfFiller
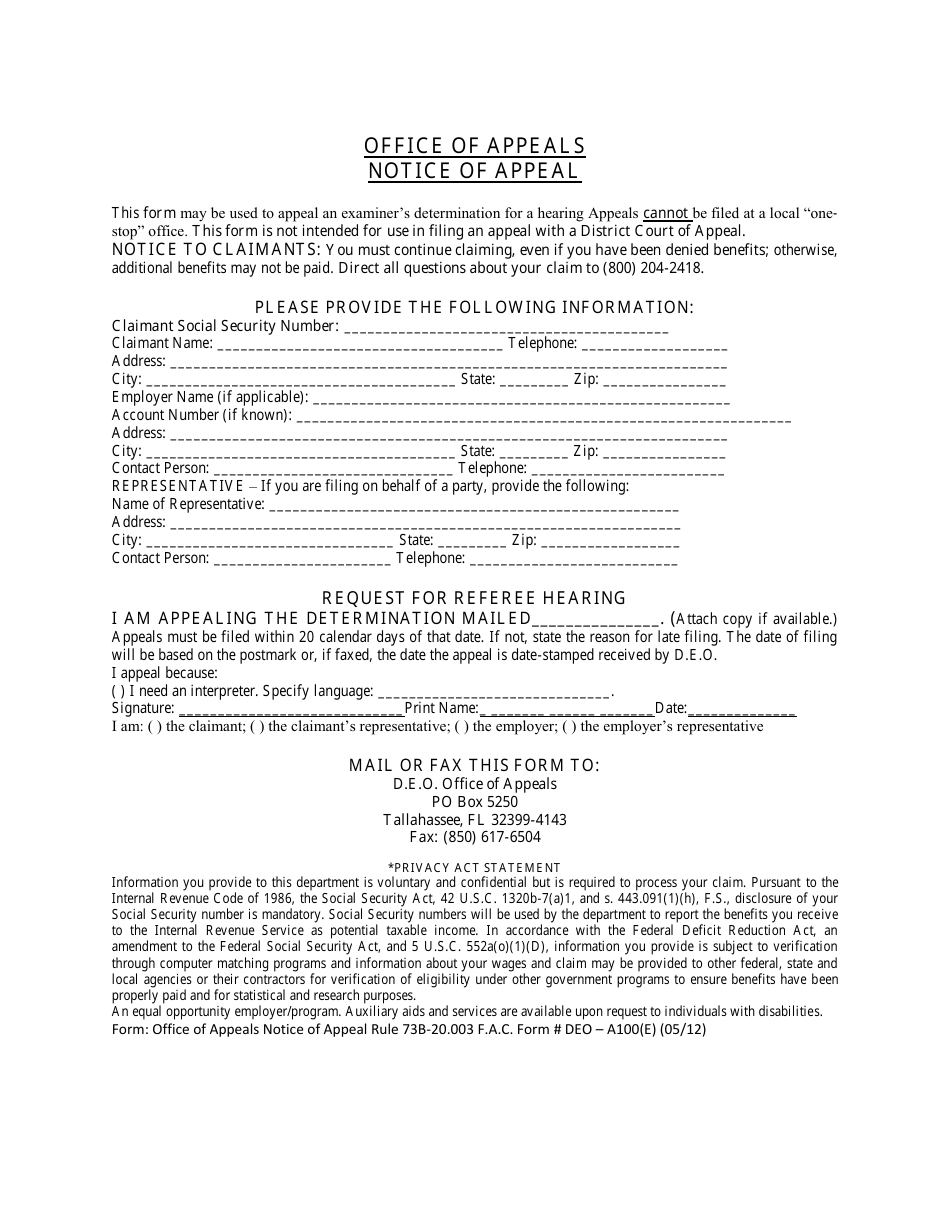
Form DEOA100(E) Download Printable PDF or Fill Online Notice of Appeal
Nics Voluntary Appeal Form eversilicon

2016 CA OSHAB Appeal Form 100 Fill Online, Printable, Fillable, Blank
Related Post: