Adventhealth Medical Records Request Form
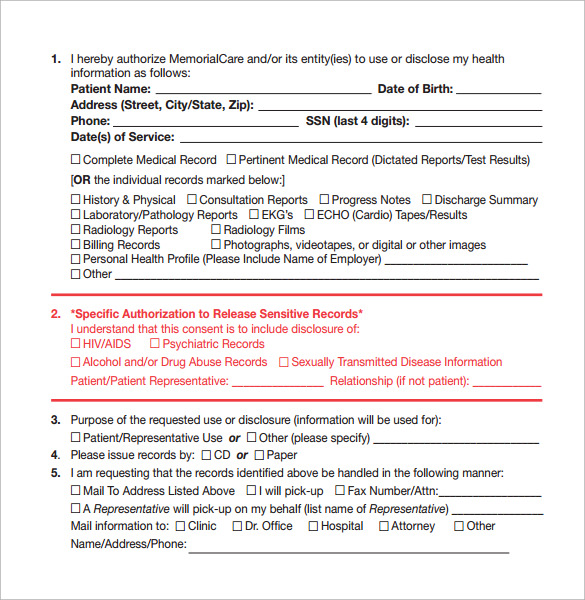
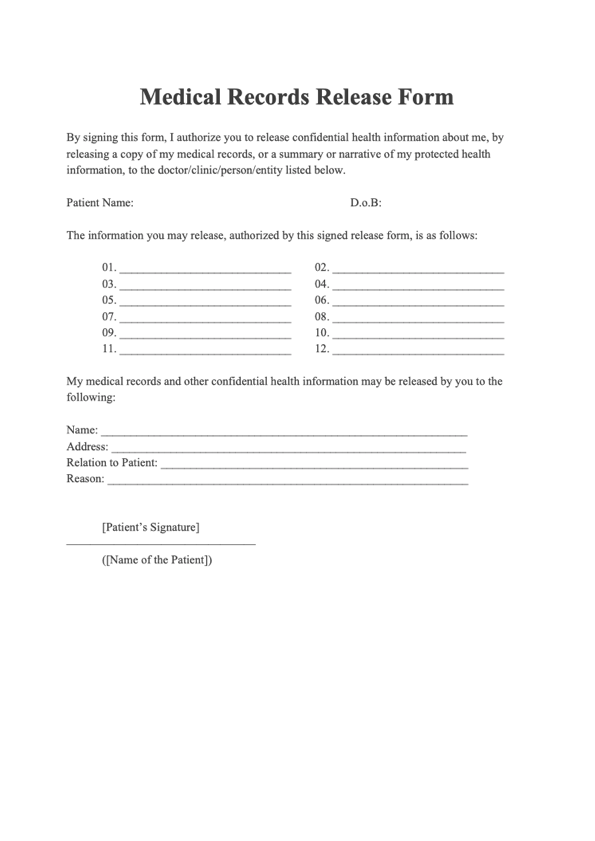
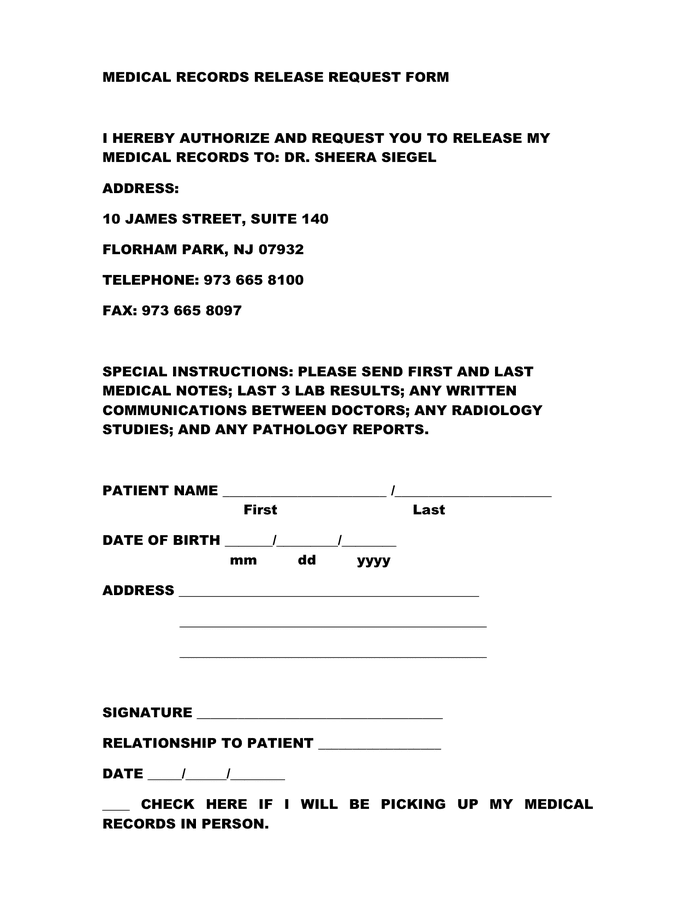
Adventhealth Medical Records Request Form - On each link you will find detailed instructions on how to. Web here are a few: Web requests should be sent from your insurance company, attorney, or disability determination service (dds) and mailed to the address on the authorization form. Web request access and/or disclosure of records for the following dates of service: Documented in her medical records that both the complainant and her companion were. Web request access and/or disclosure of records for the following dates of service: For privacy and security reasons, some medical. Web authorize the release of my medical records dated: Web not sign this form in order to assure treatment. Web create an online patient account for a safe and simple way to access information from your electronic health record (ehr). Web for privacy and security reasons, some records will not be available online. _____(check appropriate boxes below) abstract of record (dictated reports,. (one person/organization per form) name: Web to be completed by requester: Just fill out a simple form and get verified by phone. Your medical records can be released to another facility or provider for continuity. _____(check appropriate boxes below) abstract of record (dictated reports,. _____ i request copies of my medical records: Web request access and/or disclosure of records for the following dates of service: Documented in her medical records that both the complainant and her companion were. For privacy and security reasons, some medical. Web a consent to treat form is a document verifying that patients have given their permission to receive medical services from a provider. Your medical records on myhealthone. Web to be completed by requester: _____(check appropriate boxes below) abstract of record (dictated reports,. Web for privacy and security reasons, some records will not be available online. Web request your adventhealth records online with swellbox. _____(check appropriate boxes below) abstract of record (dictated reports,. Web request access and/or disclosure of records for the following dates of service: Rotate your shoulders in a circular motion, forward and backward. Web authorize the release of my medical records dated: Web for privacy and security reasons, some records will not be available online. Ad answer simple questions to make a medical records request on any device in minutes. Web create a new account. Web find the adventist health location you received services from in the list below to request a copy. Just fill out a simple form and get verified by phone. _____(check appropriate boxes below) abstract of record (dictated reports,. Web find the adventist health location you received services from in the list below to request a copy of your medical records. Create an account for easy access to doctors, extended medical services and your health records. Adventhealth is a. Web authorize the release of my medical records dated: _____(check appropriate boxes below) abstract of record (dictated reports,. _________________________check appropriate boxes below abstract of record. Click below to read, print and sign our. On each link you will find detailed instructions on how to. Web not sign this form in order to assure treatment. (one person/organization per form) name: If requested health information is needed for a doctor’s appointment, please specify date: Your medical records on myhealthone. On each link you will find detailed instructions on how to. For privacy and security reasons, some medical. Web not sign this form in order to assure treatment. Web request your adventhealth records online with swellbox. Your medical records on myhealthone. Web for privacy and security reasons, some records will not be available online. Your medical records on myhealthone. _____(check appropriate boxes below) abstract of record (dictated reports,. Web of patient medical information form 909462 rev 11/99 page 1 of 1 patient id label hereby request and authorize: Web create a new account. For privacy and security reasons, some medical. Just fill out a simple form and get verified by phone. Web a consent to treat form is a document verifying that patients have given their permission to receive medical services from a provider. _____(check appropriate boxes below) abstract of record (dictated reports,. I understand that i may inspect or obtain a copy of the information to be used or disclosed, as provided in cfr 164.524. Web create a new account. In order to obtain a copy of your record fill out the online erequest form. On each link you will find detailed instructions on how to. For privacy and security reasons, some medical. Web request your adventhealth records online with swellbox. Web of patient medical information form 909462 rev 11/99 page 1 of 1 patient id label hereby request and authorize: (one person/organization per form) name: Web to be completed by requester: Web request access and/or disclosure of records for the following dates of service: Web here are a few: Click below to read, print and sign our. Sitting with your feet on the ground and shoulders. Picked up by _________________________________ (photo id required) mailed to: _________________________check appropriate boxes below abstract of record. Your medical records can be released to another facility or provider for continuity. Rotate your shoulders in a circular motion, forward and backward.
Medical Records Request Form download free documents for PDF, Word
FREE 12+ Medical Records Request Forms in PDF Word
Medical Record Request Template
FREE 6+ Sample Medical Record Request Forms in PDF

Printable Medical Record Request Form Template Printable Templates
Medical Records Request Form Template
FREE 12+ Medical Records Request Forms in PDF Word
Printable Medical Record Request Form Template Printable Templates
Medical Records Request Form download free documents for PDF, Word
Request Medical Records Adventhealth
Related Post:
